

We offer medical detox and multiple addiction treatment options in our
luxury treatment centres in Port Hope, Cobourg, and Ottawa.
Akathisia Treatment: Causes and Symptoms

Akathisia is a medication-induced movement disorder that creates an unbearable urge to keep moving. Your legs won't stay still. Sitting feels like torture. The restlessness hits from the inside out, and no amount of willpower makes it stop. Most cases trace back to antipsychotic side effects, though other medications can trigger them too. Effective ways of treating akathisia exist, both through medication adjustments and non-drug techniques, once the condition is properly identified.
Key Takeaways:
- Why blocking a single brain receptor triggers akathisia – and which drug classes carry the steepest risk beyond antipsychotics
- How to tell akathisia apart from anxiety, restless legs syndrome, and worsening psychiatric illness, before a misdiagnosis makes things worse
- The step-by-step treatment ladder clinicians follow, from dose adjustments to rescue medications like propranolol and mirtazapine
- Which non-drug techniques can ease the motor agitation when medication changes alone aren't enough
- Why akathisia poses a specific relapse threat during addiction recovery – and how dual-diagnosis teams navigate that risk
What Causes Akathisia in the First Place?
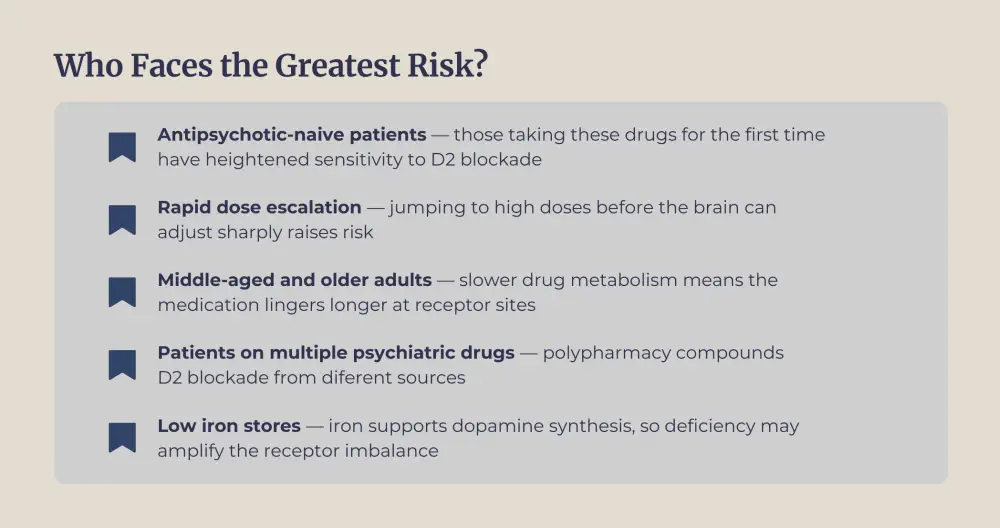
Dopamine receptor blockade in the brain drives most cases. Antipsychotic medications prescribed for schizophrenia, bipolar disorder, and other psychiatric conditions work by blocking dopamine D2 receptors. But that same D2 blockade can disrupt motor pathways, triggering the relentless urge to move that defines akathisia.

First-generation antipsychotics like haloperidol and chlorpromazine carry the steepest risk. A Canadian clinical guideline published in PMC found that community-dwelling patients with schizophrenia had an overall akathisia prevalence of 18.5%, with rates climbing to 40% among those prescribed multiple first-generation drugs. Even second-generation options aren't immune. Aripiprazole and risperidone produce higher akathisia rates than quetiapine or olanzapine.
Antipsychotic side effects aren't the only cause, though. SSRIs, anti-nausea drugs like metoclopramide, calcium channel blockers, and certain sedatives used during anesthesia have all been linked to akathisia. Cocaine and amphetamine abuse can produce similar motor agitation, which becomes especially relevant for individuals in addiction recovery who also manage co-occurring mental health conditions.
How Do You Recognize Akathisia Symptoms?
Akathisia symptoms are split into two categories: what you feel on the inside and what others can observe from the outside. The subjective experience that gnawing, crawling sense of inner restlessness can be harder to pin down than the visible fidgeting.
People describe it differently. Some say it feels like their bones are buzzing. Others compare it to an electric current running through their legs that only eases when they move. The distress goes beyond the physical. Anxiety, irritability, and a sense of emotional torment frequently accompany the motor symptoms.
Observable signs include:
- Constant shifting of weight from foot to foot
- Crossing and uncrossing legs repeatedly
- Rocking back and forth when sitting
- Pacing that the person can't seem to stop
- Fidgeting with hands, tapping, or rubbing knees
Doctors use the Barnes Akathisia Rating Scale to assess severity, measuring both the subjective complaints and the visible restlessness. Akathisia is frequently confused with anxiety, agitated depression, restless legs syndrome, or even a worsening of the psychiatric condition being treated. That misdiagnosis can lead to increased antipsychotic doses, which only makes everything worse.
The timeline matters for classification:
| Type | Onset | Duration |
|---|---|---|
| Acute akathisia | Days to weeks after starting or increasing medication | Less than 6 months |
| Chronic akathisia | Persists beyond the initial onset | Over 6 months |
| Tardive akathisia | Delayed onset, usually 3+ months after starting medication | Can persist for years |
Acute cases represent the majority. Catching them early, within those first few weeks of a new prescription, dramatically improves outcomes.

Can Akathisia Be Treated Without Stopping Your Medication?
Managing akathisia requires more than a single fix. No one intervention works for everyone, and the best results come from combining medication changes with targeted add-on therapies.
Medication-Based Relief
The first step is always re-evaluating the drug that triggered the problem. Reducing the antipsychotic dose, when clinically safe, resolves many cases on its own. If the dose can't drop further, switching to a lower-risk antipsychotic is the next move. Iloperidone carries one of the lowest akathisia risks among available options, and quetiapine at conservative doses is another common substitute.
When dose changes aren't feasible (because the patient depends on that specific medication for psychiatric stability), add-on treatments become necessary:
- Beta-blockers: Propranolol (10–20 mg, three times daily) remains the most studied and commonly prescribed rescue medication. It works by dampening the adrenergic drive behind the compulsion to move.
- Mirtazapine: At low doses (15 mg), this antidepressant has shown effectiveness comparable to propranolol in clinical trials, with a favourable side-effect profile.
- Benzodiazepines: Clonazepam or lorazepam can provide short-term relief, though long-term use raises dependency concerns, a consideration that weighs heavily for people with addiction histories.
- Anticholinergics: Benztropine helps when Parkinsonian symptoms accompany akathisia, but cognitive side effects limit its use in older adults.
- Vitamin B6: High-dose supplementation has shown some promise, though strong randomized evidence is still lacking.

How Does Akathisia Complicate Dual-Diagnosis Care?
Many individuals entering treatment for substance use disorders also carry psychiatric diagnoses – depression, bipolar disorder, PTSD, schizophrenia. Those conditions frequently require antipsychotic medication. And antipsychotic side effects like akathisia can threaten the entire path to sobriety.
What makes akathisia uniquely destructive during recovery is the overlap in sensation. The drug-induced restlessness closely resembles the internal chaos that originally fuelled substance use, and a person who once relied on alcohol or drugs to silence that agitation now confronts it courtesy of their own medication. Unsurprisingly, patients experiencing intense akathisia quit their prescribed antipsychotics at alarming rates.
Benzodiazepines, one of the standard options for treating akathisia, add another layer of concern. For someone with a history of sedative or alcohol dependence, prescribing clonazepam to manage akathisia risks trading one problem for another. This is why dual-diagnosis care requires prescribers who weigh every option against the patient's full clinical and substance use history.
FAQ
How long does akathisia last after stopping the medication?
For most people, symptoms ease within days to weeks once the triggering drug is reduced or discontinued. Tardive akathisia(the delayed-onset form) can linger for months or years after the drug is gone, because the neurological changes take longer to reverse. The speed of resolution depends heavily on how long you took the medication and at what dose.
Can akathisia be permanent?
Most cases resolve with proper akathisia treatment, but chronic and tardive forms can linger for extended periods. Permanent cases are rare and usually associated with years of high-dose antipsychotic exposure without monitoring.
Is akathisia the same as restless legs syndrome?
No. Restless legs syndrome primarily occurs at night and involves uncomfortable sensations in the legs relieved by movement. Akathisia symptoms affect the whole body, persist throughout the day, and stem from medication use, not a primary neurological condition.
What should I do if I think my medication is causing akathisia?
Contact your prescribing doctor before making any changes on your own. Stopping psychiatric medication abruptly can trigger withdrawal or psychiatric relapse. Keep a log of when symptoms started, how they feel, and how intense they get throughout the day. This information helps your doctor pinpoint the cause and choose the right adjustment.
Can antidepressants cause akathisia too?
Yes. SSRIs like fluoxetine and sertraline, along with SNRIs like venlafaxine, have been linked to akathisia, particularly, in the first few weeks after starting or after a dose bump. The risk is lower than with antipsychotics, but anyone who notices new-onset motor unease after an antidepressant change should flag it with their prescriber promptly.
Article sources
- Pringsheim, T., Gardner, D., Addington, D., et al. (2018). "The Assessment and Treatment of Antipsychotic-Induced Akathisia." Canadian Journal of Psychiatry, 63(11), 719–729. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6299189/
- Thippaiah, S.M., Fargason, R.E., & Birur, B. (2021). "Struggling to find Effective Pharmacologic Options for Akathisia? B-CALM!" Psychopharmacology Bulletin, 51(3), 72–78. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC8374932/
- Salem, H., Nagpal, C., Pigott, T., & Teixeira, A.L. (2017). "Revisiting Antipsychotic-Induced Akathisia: Current Issues and Prospective Challenges." Current Neuropharmacology, 15(5), 789–798. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC5771055/
- Poyurovsky, M., & Weizman, A. (2022). "Treatment of Antipsychotic-Induced Akathisia: Role of Serotonin 5-HT2a Receptor Antagonists." Drugs, 82(8), 871–886. Available at: https://pubmed.ncbi.nlm.nih.gov/35579806/
- Barnes, T.R.E. (1989). "A Rating Scale for Drug-Induced Akathisia." British Journal of Psychiatry, 154, 672–676. Available at: https://pubmed.ncbi.nlm.nih.gov/2574607/
- Lohr, J.B., Eidt, C.A., Alfaraj, A.A., & Soliman, M.A. (2015). "The Clinical Challenges of Akathisia." CNS Spectrums, 20(Suppl 1), 1–14. Available at: https://pubmed.ncbi.nlm.nih.gov/26683525/
- Forcen, F.E., Matsoukas, K., & Alici, Y. (2016). "Antipsychotic-Induced Akathisia in Delirium: A Systematic Review." Palliative and Supportive Care, 14(1), 77–84. Available at: https://pubmed.ncbi.nlm.nih.gov/25907412/
- Hieber, R., Dellenbaugh, T., & Nelson, L.A. (2008). "Role of Mirtazapine in the Treatment of Antipsychotic-Induced Akathisia." Annals of Pharmacotherapy, 42(6), 841–846. Available at: https://pubmed.ncbi.nlm.nih.gov/18460588/




