

We offer medical detox and multiple addiction treatment options in our
luxury treatment centres in Port Hope, Cobourg, and Ottawa.
Is Ozempic Addictive?

Ozempic is not a controlled substance, does not produce euphoria, and carries no pharmacological addiction liability. Yet stopping it can send appetite, weight, and mood into sharp reversal. That gap has confused patients and split medical opinion. The brain circuitry it targets for appetite control overlaps directly with the circuitry implicated in substance use disorders, which is why addiction specialists are watching this drug from both directions at once.
Key Takeaways
- Why Ozempic clears every clinical bar for addiction, yet some patients stopping it describe an experience that feels nothing like a clean exit.
- What the STEP 1 trial data shows about the body's trajectory once semaglutide is removed, and how fast it happens.
- Why two large studies on Ozempic and brain health reached opposite conclusions, and which one should carry more weight.
- Which four patient groups face the highest mood risk on semaglutide, and why standard prescribing assessments don't catch them.
- What a 2025 trial found when semaglutide was tested against alcohol use disorder, including an unplanned finding nobody anticipated.
Does Ozempic Meet the Clinical Definition of an Addictive Drug?
No. Ozempic addiction does not fit the clinical criteria for substance use disorder. It produces no euphoria, no escalating compulsive use, and no recognized withdrawal syndrome.
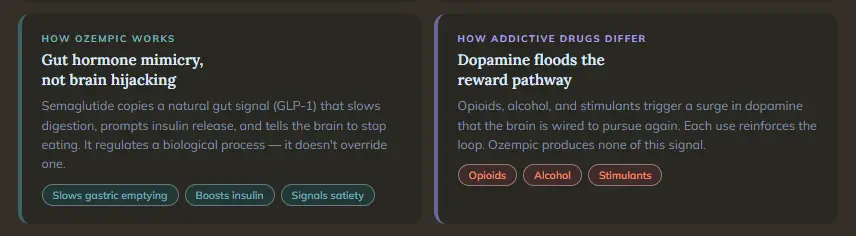
Clinicians diagnose substance use disorder when a patient takes a drug in escalating amounts to achieve the same effect, continues using it after it causes clear harm, and loses meaningful control over consumption. They reflect what happens neurochemically when a substance hijacks the brain's dopamine system, training it to crave repetition. Opioids do this. Alcohol does this. Stimulants do this with particular force. Ozempic does none of it.
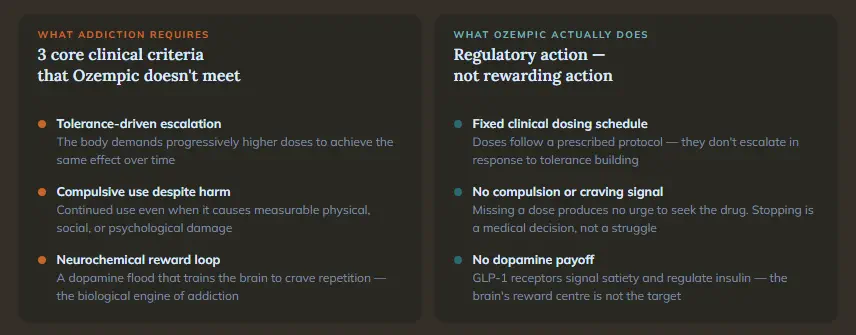
Semaglutide is a GLP-1 receptor agonist. It mimics glucagon-like peptide-1, a hormone the gut releases naturally after eating. By binding to GLP-1 receptors in the pancreas and digestive tract, it slows gastric emptying, boosts insulin secretion, and signals the brain to reduce appetite. There is no high. The drug's action is regulatory, not rewarding, which is precisely why it sits in a different pharmacological category from substances with genuine addiction liability.
The clinical definition of addiction and the lived experience of dependency are not always equivalent. Some patients report strong psychological reliance on what semaglutide produces, not on the drug itself. Fear of losing weight-loss gains, the disappearance of appetite suppression, or the return of food preoccupation after stopping can generate real distress. For someone with a history of disordered eating, that distress may feel indistinguishable from craving. It warrants clinical attention, but not a diagnosis of addiction.
The same pharmacological reasoning applies to Wegovy, Rybelsus, and all other semaglutide formulations. Ozempic vs Semaglutide covers the practical differences between branded versions.
Why Does Stopping Ozempic Feel Like Withdrawal?
Ozempic withdrawal doesn't carry a formal clinical designation, yet stopping the drug produces a cascade of physiological reversals that are neither minor nor brief.
Semaglutide has a half-life of approximately seven days. After the final dose, the drug gradually clears over several weeks, and as it does, every biological effect it was producing begins to reverse. Appetite signals return with a force that patients describe as qualitatively different from ordinary hunger. Blood sugar regulation reverts toward pre-treatment levels. Cardiovascular markers that improved on the drug, including blood pressure and cholesterol readings, regress toward baseline.
The STEP 1 trial extension tracked what happens to the body in the year after stopping. The numbers tell a consistent story of near-complete reversal.
| Measure | On Semaglutide (week 68) | One Year After Stopping |
| Average weight loss | 17.3% of body weight | Regained two-thirds |
| Blood pressure | Improved | Reverted toward baseline |
| Cardiometabolic markers | Broadly improved | Most reverted toward baseline |
A 2024 study presented at the European Congress on Obesity found that gradual dose reduction paired with active lifestyle intervention substantially reduced this rebound compared to abrupt cessation. The STEP 1 authors described obesity as a "chronic" condition with biologically defended set points that reassert themselves once regulatory support is removed, which reframes stopping Ozempic less as withdrawal and more as the uncovering of an underlying disease that was being managed, not cured.
Mood follows the same pattern. When appetite returns sharply, patients with histories of disordered eating, weight preoccupation, or body image distress can experience genuine emotional destabilization. Food cravings returning after months of quiet carry their own psychological weight. That destabilization, and not just the physical rebound, is why stopping without a medically supervised plan is not safe.
People with type 2 diabetes, comparing their medication options after stopping semaglutide, will find Ozempic vs Metformin a useful reference for what alternatives look like metabolically.

What Does Ozempic Do to Mood — and Who Is Most at Risk?
The relationship between Ozempic depression and semaglutide sits in a medically unresolved place, and that uncertainty deserves more transparency than patients routinely receive.
GLP-1 receptors are not confined to the gut and pancreas. They are present in the hypothalamus, the brainstem, and in regions that regulate dopamine transmission and emotional tone. Semaglutide acts on these areas. What that action produces varies considerably by individual.
What the Research Shows
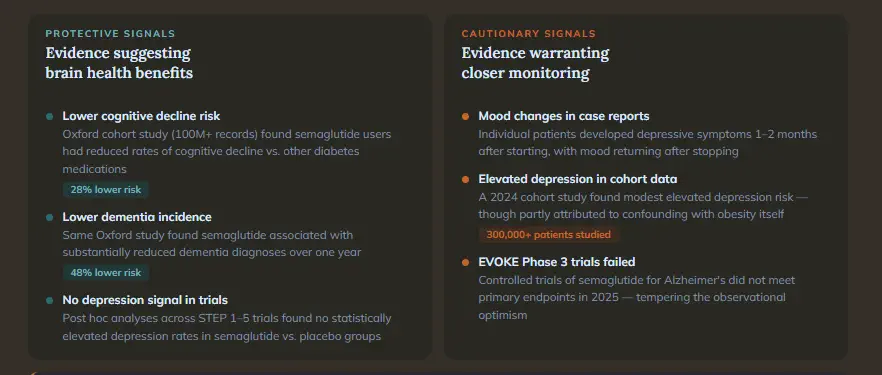
A 2024 University of Oxford cohort study using more than 100 million patient records found semaglutide users had a 28% lower risk of cognitive decline and a 48% lower risk of dementia compared to those taking other diabetes medications. Those findings apply specifically to type 2 diabetes patients and have not been replicated in controlled trials. The Phase 3 EVOKE trials, the first placebo-controlled test of semaglutide for Alzheimer's disease, did not meet their primary endpoints in late 2025. Post hoc analyses of the STEP 1 through 5 trials found no statistically elevated depression risk in the placebo-controlled setting.
On the cautionary side, case reports describe patients developing depressive symptoms one to two months after starting semaglutide, with mood improving after discontinuation. A 2024 cohort study found that those taking semaglutide had a modestly elevated depression risk compared to non-users, a finding the authors attributed partly to confounding, given that obesity itself is a depression risk. The EMA reviewed a suicidal ideation signal in July 2023 and concluded in April 2024 that available evidence did not confirm a causal link. The FDA reached the same conclusion. Both agencies continue monitoring.
Who Faces the Highest Risk
Where current prescribing guidance falls short is in identifying who sits at greatest risk of adverse mood effects. These groups warrant the closest monitoring:
- People with pre-existing low dopamine function or a history of depression
- Those taking antidepressants or antipsychotics concurrently
- Individuals in early recovery from substance use disorder
- Patients with binge-eating disorder or other eating disorders
By suppressing appetite, GLP-1 receptors may simultaneously reduce the brain's response to other pleasurable stimuli. Some patients describe this as emotional blunting or reduced motivation. For someone whose recovery depends on finding pleasure in activities, relationships, and daily life, that blunting deserves a direct conversation before the first dose.
Could the Drug Designed for Weight Loss Also Reduce Substance Cravings?
GLP-1 receptors are expressed in the nucleus accumbens and the ventral tegmental area, dopamine-rich regions that encode the salience of rewarding stimuli and drive goal-directed behaviour. That neurological overlap, between the circuitry Ozempic targets for appetite and the circuitry implicated in addiction, has been the basis of a growing body of research.
What the 2025 JAMA Psychiatry Trial Found
In February 2025, JAMA Psychiatry published results from the first randomized, placebo-controlled clinical trial of semaglutide in adults with alcohol use disorder, led by Christian Hendershot at the USC Institute for Addiction Science.
| Trial Detail | Finding |
| Design | Phase 2 RCT, 48 participants, 9 weeks |
| Alcohol craving | Significantly reduced vs. placebo |
| Drinks per drinking day | Significantly reduced vs. placebo |
| Heavy drinking days | Greater reductions vs. placebo over time |
| Effect size vs. existing AUD medications | Comparable or exceeded at low doses |
A separate 2024 observational study published in Nature Communications found that people taking GLP-1 medications had a 40% lower rate of opioid overdose and a 50% lower rate of alcohol intoxication events compared to matched controls. The proposed explanation is consistent across both studies. Semaglutide may reduce the motivational pull of addictive substances by the same pathway it quiets the pull of food. An addictive trigger becomes less compelling not because the person has resolved what drives the craving, but because its neurological amplification has been dampened.
The Hendershot trial also found semaglutide predicted greater reductions in cigarettes per day among participants who smoked, an unplanned finding that extends the reward-suppression hypothesis beyond alcohol alone.
Why Caution Still Applies
The trial results are promising. They are not a green light for off-label prescribing in addiction populations:
- Semaglutide carries no FDA approval for addiction treatment
- The Hendershot trial used only low doses and ran for nine weeks
- Phase 3 trials are underway but not yet complete
- Long-term safety data in addiction populations does not exist
- Off-label prescribing is happening without standardized protocols
Structured, medically supervised residential treatment remains the gold standard for substance use disorders. Pharmacological aids can support recovery, but they cannot replicate the therapeutic work of addressing the psychological, relational, and environmental conditions that sustain addiction. The Canadian Centre for Addictions provides evidence-based residential programs for people with substance use disorders, including those with co-occurring medical conditions like obesity or type 2 diabetes.
What Are the Side Effects of Ozempic That Patients Overlook?
The nausea is well-documented. The side effects of Ozempic that receive less attention are those appearing gradually, sometimes weeks or months into treatment, becoming more pronounced during dose escalation or after stopping.
Gastrointestinal Effects
Nausea, vomiting, constipation, and slowed gastric emptying affect a majority of new users during the initial dose-escalation phase. For most, these diminish over several weeks, though persistent GI effects can interfere with adequate nutrition.
The Body Composition Problem
In the STEP 1 trial, approximately 40% of the total weight lost was lean mass, not fat. Patients who stop semaglutide and regain weight tend to regain fat more readily than muscle, which can leave them with a worse body composition ratio than before they started. Resistance training during treatment reduces this outcome and is increasingly recommended as a clinical co-intervention.
Cognitive and Mood Complaints
Difficulty concentrating, mental fogginess, and reduced motivation are reported frequently enough to constitute a signal worth noting. Clinical trials did not list these as confirmed side effects, and the Oxford cohort study found semaglutide associated with reduced cognitive decline risk over time. The real-world complaints likely reflect the trials' exclusion of patients with psychiatric histories. For people in addiction recovery, a drug that blunts pleasure-seeking is not neutral, and that conversation is best had before the prescription is written.

What Should You Know Before Starting or Stopping Ozempic?
Stopping abruptly carries a steep physiological cost. A supervised taper paired with resistance training preserves more of the drug's gains than any other exit the research has identified.
Patients on psychiatric medications, those in addiction recovery, and anyone with a history of eating disorders or low mood carry a distinct neurological profile that standard prescribing assessments don't capture. Their prescriber and addiction specialist should be communicating before the first dose, not after problems emerge.
The 2025 JAMA data on alcohol use disorder are among the most compelling early signals in addiction pharmacology in years. It is also a phase 2 trial with 48 participants. It justifies the phase 3 trials now underway. It does not justify treating Ozempic as an addiction therapy today. Good addiction treatment is medically supervised, psychologically supported, and built around the individual's full history.
If you or someone close to you is dealing with substance use alongside complex medical conditions, call the Canadian Centre for Addictions at 1-855-499-9446 for a free, confidential consultation.
FAQ
Will Ozempic show up on a drug test?
No. Semaglutide is not a controlled substance in Canada and is not screened for in standard workplace or forensic drug panels. Standard urine or blood drug tests do not detect it.
Can someone on methadone or Suboxone take Ozempic?
Potentially, but this requires direct coordination between the prescribing physician and the addiction medicine team. Both semaglutide and opioid agonist therapies affect appetite, metabolism, and GI function, and their combined effects need active monitoring from clinicians who know about both prescriptions.
Is Ozempic covered by provincial health insurance in Canada?
Coverage varies by province and by diagnosed indication. In Ontario, semaglutide (Ozempic) is listed on the Ontario Drug Benefit formulary for type 2 diabetes under specific criteria. Weight loss indications are not publicly covered in most provinces and require private insurance or out-of-pocket payment.
Is it safe to take Ozempic during pregnancy or when planning to conceive?
No. Ozempic is contraindicated during pregnancy. Most prescribers advise stopping semaglutide at least two months before trying to conceive, given its half-life of approximately seven days and the absence of adequate fetal safety data.
If Ozempic reduces food cravings, could it help someone in recovery avoid cross-addiction to food or sugar?
This is an area of active clinical interest with no formal guidance yet. Anecdotal reports describe reduced compulsive eating in people on semaglutide, and the reward-pathway biology is plausible, but no controlled studies have examined this specifically in substance use recovery populations. Anyone considering it for this purpose should discuss it with both a physician and an addiction specialist before making any decision.
Article sources
- Wilding, J.P.H., et al. "Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension." Diabetes, Obesity and Metabolism. 2022. https://dom-pubs.onlinelibrary.wiley.com/doi/10.1111/dom.14725
- Wang, W., et al. "Associations of semaglutide with incidence and recurrence of alcohol use disorder in real-world population." Nature Communications. 2024;15(1):4548. https://www.nature.com/articles/s41467-024-48780-6
- Wadden, T.A., et al. "Psychiatric safety of semaglutide for weight management in people without known major psychopathology: post hoc analysis of the STEP 1, 2, 3, and 5 trials." JAMA Internal Medicine. 2024. https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2816801
- European Medicines Agency. "Meeting highlights from the Pharmacovigilance Risk Assessment Committee (PRAC) 8-11 April 2024." https://www.ema.europa.eu/en/news/meeting-highlights-pharmacovigilance-risk-assessment-committee-prac-8-11-april-2024
- Taquet, M., et al. "12-month neurological and psychiatric outcomes of semaglutide use for type 2 diabetes: a propensity-score matched cohort study." eClinicalMedicine. 2024. https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(24)00305-5/fulltext
- Novo Nordisk. "Semaglutide fails to slow cognitive decline in early Alzheimer's: EVOKE Phase 3 data." Medscape. November 2025. https://www.medscape.com/viewarticle/semaglutide-fails-slow-cognitive-decline-early-alzheimers-2025a1000wsz
- Jaiswal, D., et al. "Psychiatric side effects of GLP-1 receptor agonists: A systematic review and meta-analysis." Diabetes Research and Clinical Practice. 2023;204:110904. https://pubmed.ncbi.nlm.nih.gov/37648318/ /a>




