

We offer medical detox and multiple addiction treatment options in our
luxury treatment centres in Port Hope, Cobourg, and Ottawa.
What Is Molly? Effects and Dangers

"Molly" gets marketed as the cleaner, purer version of a party drug, and that reputation is almost entirely fiction. The street name is short for "molecular," referring to the powder or crystal form of 3,4-methylenedioxymethamphetamine(MDMA). Capsules reaching users carry synthetic cathinones, fentanyl, methamphetamine, and other adulterants at rates that make the original compound almost incidental. The marketing around it has always outpaced the reality.
Key Takeaways:
- Why the purity reputation around Molly vs MDMA is a marketing claim rather than a chemical reality – and what harm reduction lab tests find inside most capsules instead
- How this compound hijacks three neurotransmitter systems at once, and why that combination produces a crash that outlasts the high by days
- Which Molly effects are well-documented – and which concurrent physical responses most users don't notice until they've already become dangerous
- What repeated use does to verbal memory, cardiovascular health, and mood stability over months and years of use
- Why a comedown and true Molly withdrawal are clinically different conditions – and what the distinction means for how long recovery actually takes
What Exactly Is Molly, and Why Is the Name Misleading?
Molly is a street name for MDMA sold in powder or crystal form, sold loose in gel capsules or small plastic bags. Its supposed selling point is purity – no binders, no pressed tablets, no adulterants. That claim has always been dubious, and lab data makes it worse. Harm reduction organisations testing street samples have found that a substantial share of capsules sold as Molly contain little to no actual compound, replaced instead by synthetic cathinones (commonly called bath salts), caffeine, methamphetamine, or, increasingly, fentanyl.
Why Adulterants Change the Risk Profile Entirely
This matters for reasons that go beyond simple fraud. Synthetic cathinones produce dramatically different physiological responses than the entactogen, more paranoia, more aggression, more dangerous hyperthermia, and users have no way of knowing which substance they've actually taken until Molly symptoms start appearing. Fentanyl contamination raises the stakes further. A dose calibrated for the substance becomes potentially lethal when the capsule contains an opioid with a fraction of the lethal threshold.
How Canadian Law Classifies the Compound
The Molly vs MDMA distinction gets treated as meaningful in party culture, but Canada's Controlled Drugs and Substances Act classifies the drug as a Schedule III restricted drug, the same category as LSD and psilocybin, with no approved medical use outside of closely supervised research exemptions. The name on the capsule has no bearing on the contents, the legal consequences, or what the body absorbs after ingestion.
The name on the capsule has no bearing on the contents, the legal consequences, or what the body absorbs after ingestion. For a full breakdown of how the two forms compare in purity, composition, and risk, ourarticle “How Molly differs from ecstasy” covers the distinction in detail.
What Does Molly Do to the Brain?
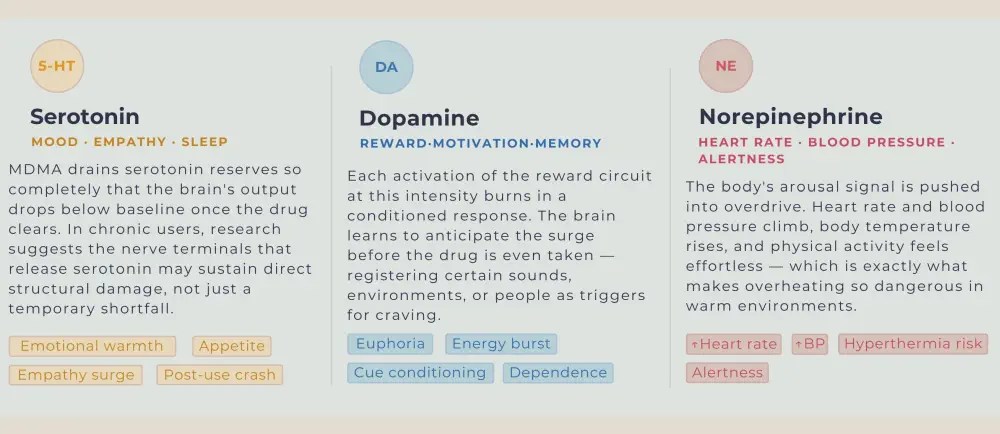
MDMA hijacks three neurotransmitter systems simultaneously. Serotonin governs mood, empathy, sleep, and appetite. Dopamine drives the brain's reward and motivation circuits. Norepinephrine regulates heart rate, blood pressure, and the body's stress response.
What does Molly do that most substances don't? It floods all three systems at once, producing an experience of warmth, connection, and energy that feels qualitatively different from alcohol or cannabis.
That intensity is pharmacologically earned, but at a cost the body can't absorb cleanly.
Serotonin surges to levels the brain cannot sustain, and research on chronic users suggests the drug may directly damage the axon terminals of serotonin-producing neurons. Unlike simple depletion, which corrects itself within days, axonal damage takes considerably longer to repair, and in heavy users, may not fully reverse. That's why the mental health fallout from repeated use isn't proportional to the dose; it accumulates.
Dopamine's role is subtler but equally consequential. Each time the reward circuit fires at that intensity, it encodes a memory trace that becomes difficult to override. The brain starts cataloguing the cues, particular music, a specific venue, a group of friends, and associating them with the expectation of that dopamine surge. Psychological dependence takes root here, well before any formal addiction pattern is visible to the person or the people around them.
What Are the Short-Term Molly Symptoms and Effects?
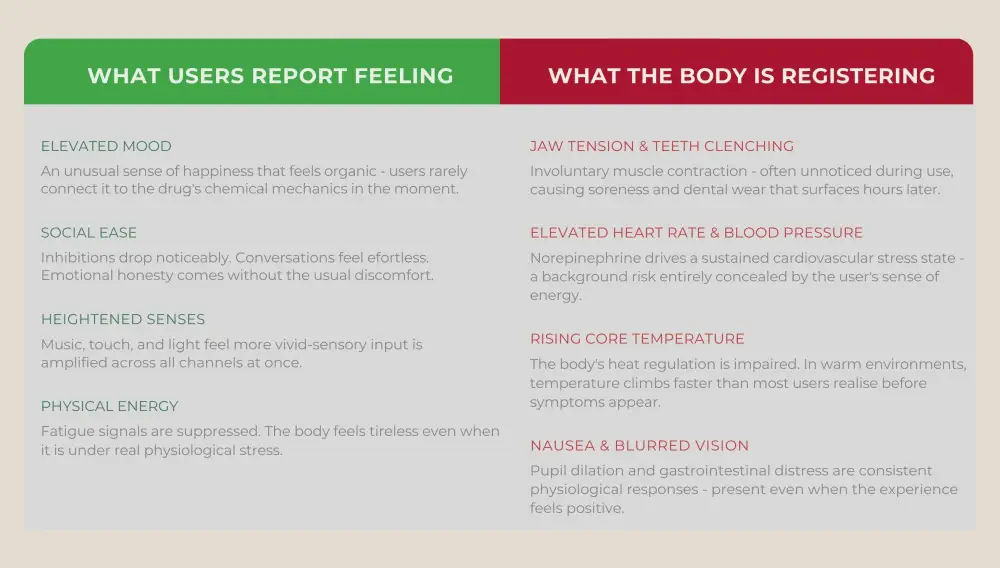
The desired love drug effects are euphoria, heightened sensory perception, emotional openness, reduced social inhibition, onset within 30 to 45 minutes of ingestion, and lasting three to six hours. The high itself is well-documented. What gets underreported are the concurrent Molly symptoms that run alongside it, particularly the ones that turn dangerous in specific environments.
Hyperthermia is the most medically serious short-term risk. The substance elevates core body temperature directly, and sustained physical activity in a warm environment (a club, a festival, a crowded venue) can push that temperature high enough to cause organ failure. Kidney damage, liver damage, and cardiac arrest have all been documented in cases where hyperthermia went unrecognised and untreated. This is not a rare edge case; it accounts for the majority of MDMA-related deaths.
Serotonin Syndrome and Hyponatremia
Serotonin syndrome is a separate but equally serious risk, particularly for anyone taking SSRIs, SNRIs, or other serotonergic medications. The syndrome presents as agitation, rapid heart rate, high fever, muscle rigidity, and, in severe cases, seizures. It can appear quickly and requires emergency medical attention. Jaw clenching, elevated blood pressure, nausea, and blurred vision are common enough that most users encounter them; serotonin syndrome and hyponatremia (dangerously low sodium from drinking excessive water to combat dehydration) belong in a different category of severity entirely.
What Are the Long-Term Dangers of MDMA Use?
Cognitive damage accumulates with repeated use in ways that aren't immediately visible. Research on heavy users of the compound consistently identifies deficits in verbal memory, attention span, and the speed at which the brain absorbs new information. These aren't subtle statistical findings – people who've used heavily over the years report noticeable difficulty retaining information and concentrating on tasks that previously required no effort.
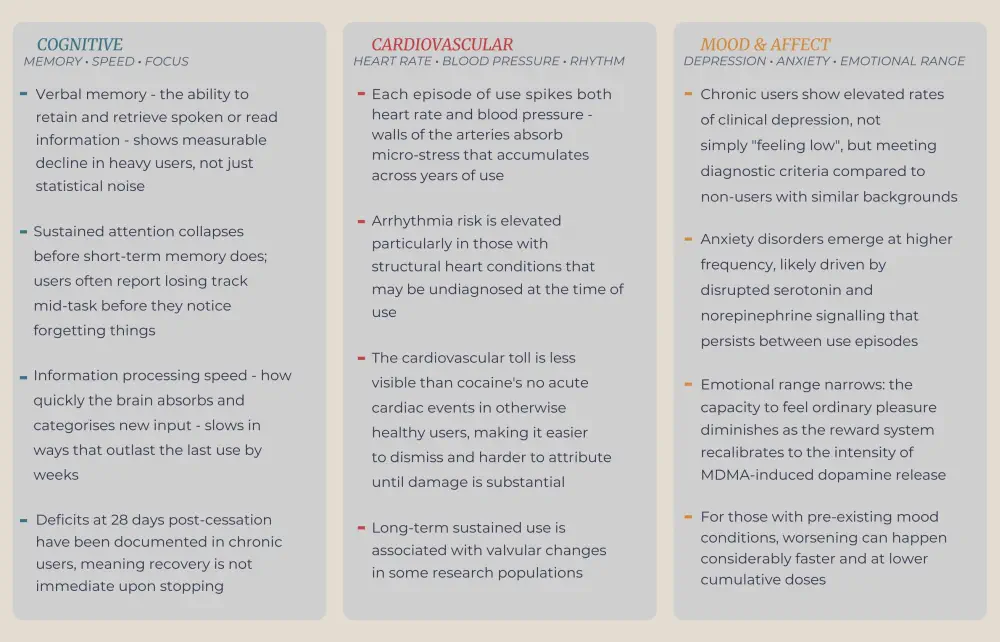
The mental health consequences connect directly to the serotonin depletion described earlier. Each heavy use episode depletes serotonin reserves and, over time, may damage the neurons that produce and receive it. Chronic users face elevated rates of depression and anxiety disorders, and people who already live with mood conditions are at particular risk of worsening. The self-medication trap is real here: someone using this substance to cope with low mood accelerates the very neurological damage that deepens that low mood.
Cardiovascular effects accumulate quietly. Repeated spikes in blood pressure and heart rate stress the arterial walls over the years, and there is a documented risk of arrhythmia in people with certain pre-existing heart conditions. The compound is not the drug that produces immediate cardiac events in otherwise healthy people with the regularity of, say, cocaine, but the cumulative toll of sustained use on the cardiovascular system is real and underappreciated.
The Dependency Pattern That Hides Itself
Dependency on this compound is less physically acute than with opioids or alcohol, but the pattern of use that precedes it is easy to miss precisely because it doesn't look like classical addiction. It tends to manifest as escalating weekend use – higher doses needed each time, longer recovery periods between sessions, and social life increasingly structured around access to the drug. Because there's no daily use and no dramatic physical withdrawal in the early stages, many people don't identify it as dependency until the recovery periods stop working for anyone ready to examine what addiction treatment actually involves. At that stage, the earlier the recognition, the more straightforward the path forward.
What Does Molly Withdrawal Actually Look Like?
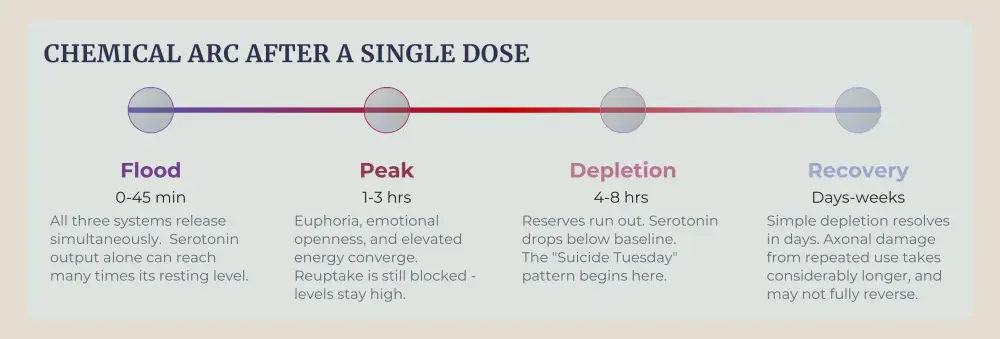
A comedown and Molly withdrawal are not the same thing, though the distinction rarely gets explained clearly. A comedown is the crash that follows a single episode of use – 24 to 72 hours of depression, exhaustion, irritability, and difficulty sleeping as serotonin levels try to recover. This happens to virtually everyone who uses the substance, regardless of how frequently.
The condition is different: it results from repeated, heavy use and reflects the brain's adaptation to chronic serotonin and dopamine disruption.
The First 72 Hours
During the first 24 to 72 hours of withdrawal from the drug, the neurochemical deficit hits hardest. Depression can be severe, not simply flat. Fatigue reaches the point where ordinary tasks feel unmanageable. Insomnia arrives alongside the exhaustion, compounding it. Cravings are strongest at this stage. The colloquial term "Suicide Tuesday" used to describe the depression that settles in two to three days after a weekend of heavy use captures how acute the mood crash can become, and it's worth taking seriously as a clinical concern, not dismissing it as dark humour.
Week One and the Recovery Timeline for Mood
From days four to ten, physical symptoms begin to ease. The emotional picture takes longer. Anxiety, difficulty concentrating, mood swings, and a general sense of anhedonia can persist for two to four weeks in people who've used heavily over a sustained period. Memory and attention problems have been documented for up to 28 days post-cessation in chronic users. Serotonin levels may take weeks to months to return to baseline, which means the recovery timeline for mood is considerably longer than the timeline for physical discomfort.

Can a Drug Be Both a Medical Candidate and a Street-Level Risk at the Same Time?
MDMA occupies an unusual position in the current drug landscape. In August 2024, the FDA formally declined to approve MDMA-assisted therapy for PTSD. Two Phase 3 trials had shown clinically meaningful symptom reduction, yet the agency cited concerns about trial integrity, cardiovascular risks, and the drug's potential for abuse.
That decision reflects something worth sitting with – regulators couldn't clear it even under controlled clinical conditions with trained therapists present and cardiac monitoring in place. On Canadian streets, the same compound arrives in unlabelled capsules of unknown composition, taken in crowded venues without any of those safeguards. The gap between those two realities is where most of the harm lives.
FAQ
Is Molly the same thing as MDMA or ecstasy?
Both are street names for MDMA, the same synthetic compound. The powder or crystal form is sold in capsules; ecstasy refers to pressed tablets, but both are routinely adulterated, and neither is reliably pure.
How long do Molly effects last?
Molly's effects onset within 30 to 45 minutes and last three to six hours, with duration shaped by dose, individual metabolism, and other substances taken at the same time. The comedown period, characterised by fatigue, low mood, and difficulty sleeping, can persist for one to three days afterward.
What are the most dangerous Molly symptoms to watch for?
Watch for someone who stops sweating in a hot environment, becomes confused, moves with unusual rigidity, or loses consciousness. These signals hyperthermia or serotonin syndrome. Extreme thirst after heavy water intake points to hyponatremia. All three escalate fast; call emergency services immediately.
How long does Molly's withdrawal last?
The acute phase of Molly withdrawal, the worst of the depression, fatigue, and cravings, runs from 24 to 72 hours for most people. Psychological symptoms like anxiety, mood instability, and difficulty concentrating can persist for two to four weeks in heavy users, and cognitive effects have been documented for up to a month.
Can you become addicted to MDMA?
This dependency pattern doesn't fit the daily-use model most people associate with addiction. It tends to be escalating weekend binges, with higher doses needed each time and longer recovery periods after each session. Most people don't recognise it as a problem until the recovery periods stop working.
What should you do if someone is having a bad reaction to Molly?
Move them somewhere cool, keep them calm, and call emergency services immediately if there are signs of overheating, confusion, chest pain, or seizures. Do not leave them alone, do not give them more water than small sips unless directed by emergency staff, and tell paramedics exactly what was taken and when.
Article sources
- National Institute on Drug Abuse. MDMA (Ecstasy/Molly). 2024. Available at: https://nida.nih.gov/research-topics/mdma-ecstasy-Molly
- Kalant H. The pharmacology and toxicology of "ecstasy" (MDMA) and related drugs. CMAJ. 2001;165(7):917–928. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC81503/
- White CM. How MDMA's pharmacology and pharmacokinetics drive desired effects and harms. J Clin Pharmacol. 2014;54(3):245–252. Available at: https://pubmed.ncbi.nlm.nih.gov/24114787/
- Papaseit E, Pérez-Mañá C, Torrens M, et al. MDMA interactions with pharmaceuticals and drugs of abuse. Expert Opin Drug Metab Toxicol. 2020;16(5):357–369. Available at: https://pubmed.ncbi.nlm.nih.gov/32216428/
- Rigg KK, Sharp A. Deaths related to MDMA (ecstasy/Molly): prevalence, root causes, and harm reduction interventions. J Subst Use. 2018;23(4):345–352. Available at: https://pubmed.ncbi.nlm.nih.gov/29910701/
- Palamar JJ, Salomone A, Massano M, Cleland CM. Trends in reported and biologically confirmed drug use among people who use ecstasy in the nightclub/festival-attending population, 2016–2022. Drug Alcohol Depend Rep. 2023;9:100198. Available at: https://pubmed.ncbi.nlm.nih.gov/37920766/




