

We offer medical detox and multiple addiction treatment options in our
luxury treatment centres in Port Hope, Cobourg, and Ottawa.
Polysubstance Abuse: What It Is, Its Dangers, and Effects

Between 2014 and 2017, the rate of substance poisoning deaths in Canada nearly doubled, climbing from 6.4 to 11.5 per 100,000 people. Poly substance use is not a single reckless night, but a recurring pattern where two or more drugs collide inside the body with effects no one can fully predict. Prescription drug abuse plays an increasingly visible role in these numbers, as medications once considered safe get mixed with alcohol, street drugs, or each other.
Key Takeaways:
- How poly substance use differs from single-drug misuse – and the surprisingly common ways people slide into it without realizing the danger
- Why mixing substances creates risks that go far beyond what either drug would do alone, including the specific combinations behind most overdose deaths in Canada
- What polysubstance abuse does to your body and brain in the short term, and the damage that builds quietly over months and years
- Which populations face the steepest risks – from high school students combining four substances at once to seniors whose prescription lists have grown unchecked
- The behavioural and physical warning signs that point to polydrug abuse rather than a single-substance problem
What Is Poly Substance Use and How Does It Start?
Polydrug use means consuming two or more drugs within the same period, be it hours apart or simultaneously. When that pattern becomes compulsive, disrupts daily functioning, and damages health, clinicians classify it as polysubstance use disorder.
People land here through different doors. Some chase a stronger high by stacking substances. Others try to counteract side effects using a stimulant to shake off sedation, or a depressant to calm a stimulant's jittery edge. Tolerance plays a role, too. When one substance stops delivering the expected effect, adding a second or third substance seems like a logical fix, even when it makes everything more dangerous.
People who use drugs consume an average of 2.6 to 4.0 different substances. And not all of it is deliberate. Prescription drug abuse feeds into polysubstance patterns quietly. Someone takes a prescribed benzodiazepine, has wine with dinner, and doesn't realize they've just doubled down on central nervous system depression.
What Makes Polysubstance Use Disorder So Dangerous?
Drug interactions don't work like simple math. Two sedatives at half-strength don't produce one full dose of sedation. They can trigger a synergistic reaction several times stronger than expected. That gap between what users anticipate and what their body actually experiences is where overdoses happen.
Stimulants and depressants pull the body in opposite directions at once. The stimulant masks the warning signs of overdose. Heart rate stays elevated. Breathing seems fine. Then the stimulant wears off, and the full weight of the depressant crashes through without warning. That delayed reaction kills people who genuinely believed they were handling it.
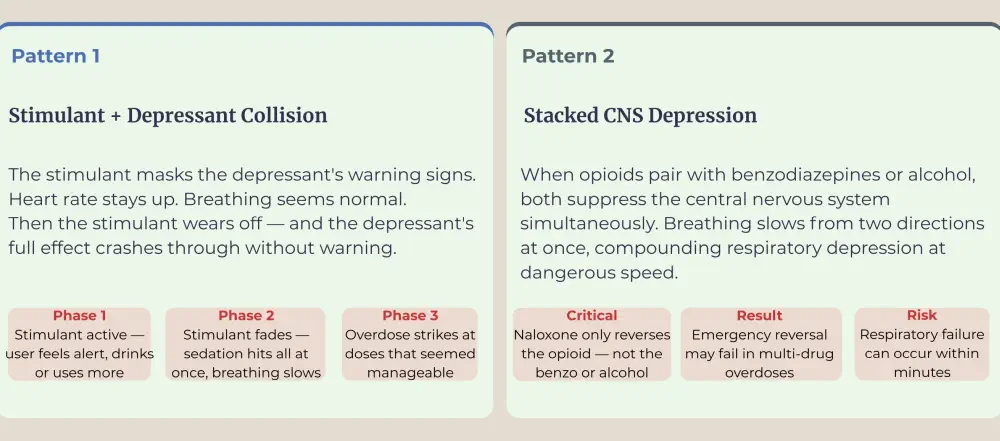
Opioids combined with benzodiazepines compound respiratory depression at a terrifying speed. The CDC's State Unintentional Drug Overdose Reporting System found that nearly half of all drug overdose deaths involved multiple substances.
Common High-Risk Combinations
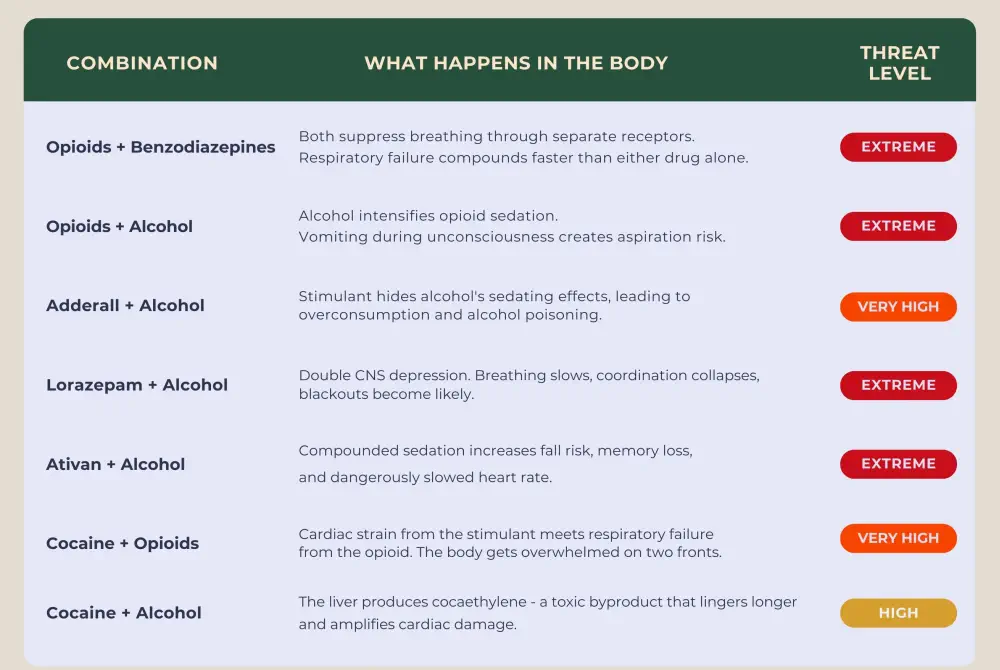
Certain drug pairings carry outsized risk. Adderall and alcohol create a dangerous mismatch; the stimulant hides alcohol's sedating effects, leading people to drink far more than their body can safely handle. Lorazepam and alcohol both depress the central nervous system at the same time, slowing breathing, collapsing coordination, and making blackouts likely. A similar collision happens when mixing alcohol and Ativan, where compounded sedation raises the risk of falls, memory loss, and dangerously slowed heart rate. Opioids paired with stimulants attack the body from opposite directions. Cardiac strain from the stimulant meets respiratory failure risk from the opioid, overwhelming two organ systems at once.
What are the Short-Term and Long-Term Effects of Multiple Substance Use?
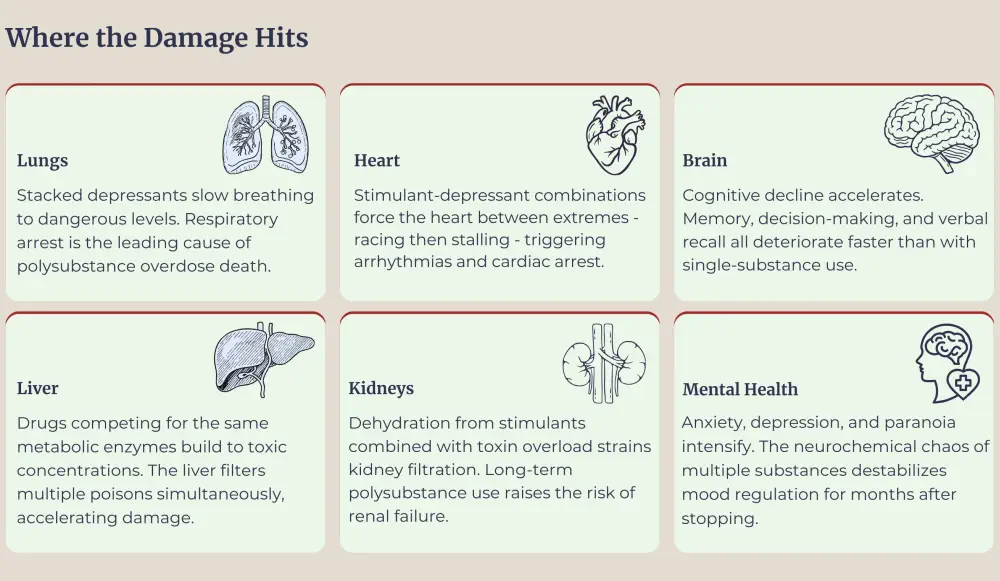
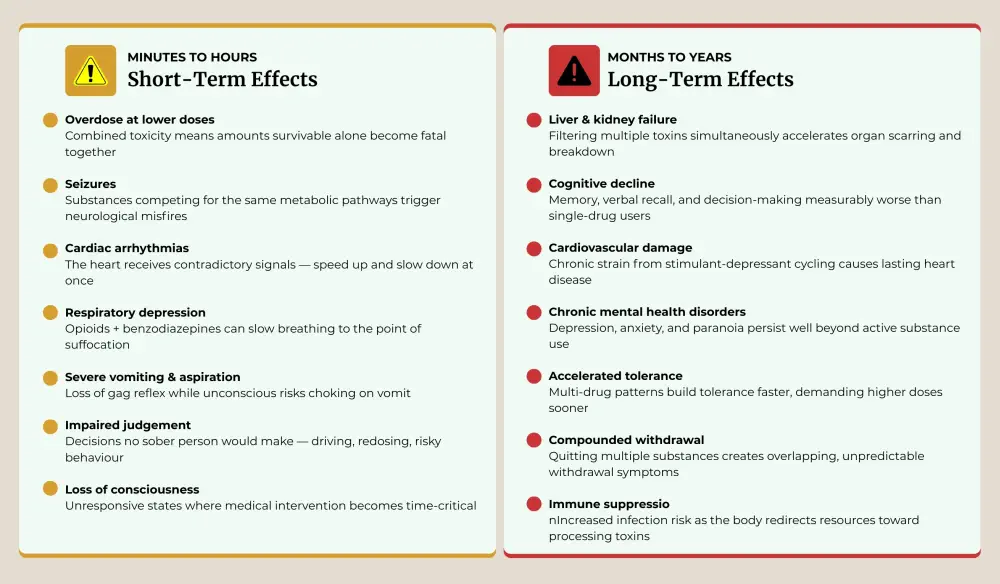
Short-term consequences hit fast and hard. Overdose can occur at doses that would be survivable with a single drug; combined toxicity means your body takes on more poison than either substance would generate alone. Seizures, cardiac arrhythmias, severe vomiting, and loss of consciousness all escalate when substances compete for the same metabolic pathways. Impaired judgement compounds the danger; people make decisions they'd never consider sober, from driving to taking additional doses.
Long-term damage accumulates quietly. The liver and kidneys are strained by the burden of filtering multiple toxic substances. Cognitive decline sets in. Research using the California Verbal Learning Test found that polysubstance users performed worse on memory and recall tasks than those using alcohol alone, suggesting that mixing drugs accelerates brain damage beyond what any individual substance would cause.
Abusing prescription medications creates a specific wrinkle here. Many prescribed medications(opioids, benzodiazepines, certain antidepressants) compete for the same liver enzymes during metabolism. When two drugs need the same enzyme to break down, one metabolizes more slowly, building to toxic concentrations in the bloodstream. A dose that's perfectly safe on its own becomes poisonous when paired with the wrong second substance.
H2: Who Is Most at Risk for Polysubstance Use Disorder?
Certain populations carry a higher risk than others. People managing chronic pain through opioid prescriptions are particularly vulnerable — adding a benzodiazepine for anxiety or a muscle relaxant for spasms creates a multi-drug regimen that can turn dangerous without anyone intending harm. Older adults face compounding risk from polypharmacy, where five or more daily medications slow each other's metabolism and amplify side effects.
Younger adults experimenting in social settings rarely understand interaction risks. A drink at a party, a friend's prescription pill, plus a line of cocaine might seem like three separate choices. Biologically, it's one dangerous event.
The unregulated drug supply adds another layer of risk that's impossible to control. Fentanyl contamination means people using stimulants may unknowingly ingest opioids. Canada lost an average of 20 people per day to opioid-related overdoses in 2024, with many of those deaths involving multiple substances.

Polysubstance Abuse in Young Adults
Among Canadian students in grades 7 through 12, the CSADS 2023-24 survey recorded 18% reporting polysubstance use in the past year. That rate increases steeply with age, from 7% in Grade 7 to 33% in Grade 12. The COMPASS longitudinal study tracking high school students between 2013 and 2018 confirmed the trend was accelerating year over year, with the steepest rise appearing in quad-substance use — students combining alcohol, cigarettes, cannabis, and e-cigarettes all at once.
Here's a counterintuitive finding from the CSADS: 13% of Grade 7 students believed polysubstance use posed little to no risk, compared to just 7% of Grade 12 students. The youngest cohort, with the least experience, was the most dismissive of danger and the most likely to stumble into harmful combinations without grasping what they'd done.
Who bears the heaviest burden:
- Rural students. Health Canada found polysubstance use rates of 24% in rural areas versus 17% in urban settings. Fewer harm reduction resources, limited counselling access, and smaller social networks where substances pass more freely between the same group of friends all feed the gap.
- Male and Indigenous students. The COMPASS study found both groups were significantly more likely to engage in multi-substance use compared to female and white students — a disparity that widened over the study period.
- Postsecondary students. After high school, the numbers climb further. 26% of university and college students reported polysubstance use in the past 12 months. Among those combining substances, 74% paired alcohol with cannabis, by far the dominant combination. Prescription stimulants taken to power through exams get paired with alcohol or cannabis hours later to wind down, normalizing a polydrug cycle that started as a productivity strategy.
The mental health fallout from these patterns is measurable. Regular use of two substances was associated with significantly more frequent anxiety symptoms. But the specific combination mattered: the cannabis-nicotine pairing showed the strongest link to both anxiety and reduced positive mental health, while other pairings produced different risk profiles. That specificity carries weight for treatment planning – it's not just how many substances someone uses, but which ones they combine.
Polysubstance Abuse in Older Adults

Roughly 27% of Canadian seniors take five or more medications daily, with prevalence estimates reaching as high as 66% depending on the study population. In Quebec, a third of community-dwelling older adults were taking ten or more prescribed medications as of 2022. That same Quebec population study found nearly half of all older adults on medication faced at least one indicator of potentially inappropriate polypharmacy – a harmful drug-drug interaction, a medication considered unsafe for elderly patients, or a prescription carrying a high anticholinergic burden.
The anticholinergic piece often gets missed. Medications with anticholinergic properties(certain antihistamines, bladder drugs, tricyclic antidepressants, and some antipsychotics) accumulate their cognitive effects when stacked. A patient taking two or three of these medications simultaneously can develop confusion, blurred vision, or delirium that gets chalked up to aging when it's really a drug burden problem.
Cognition declines with each medication added. A 2024 meta-analysis of 27 studies covering over 124 million older adults found that polypharmacy (five or more medications) increased the risk of cognitive impairment by 39%, while excessive polypharmacy (ten or more) raised that risk by 51%. The pattern is consistent across populations and study designs: more medications correlate with more rapid cognitive decline, even in adults whose underlying health conditions are well managed.
Where traditional polysubstance discussions don't fit older adults:
- The prescriber is often part of the problem. Multiple specialists writing prescriptions independently( a cardiologist, a rheumatologist, a psychiatrist) may each add a reasonable medication without anyone reviewing the full list. The patient fills every script. The pharmacy software flags a few interactions. Nobody acts on the flags.
- Over-the-counter products fly under the radar. NSAIDs, antihistamines, melatonin, herbal supplements – older adults add these without telling their doctors, not out of secrecy but because they don't consider them "medications." Yet each one can amplify or interfere with prescription drugs already on the list.
- Alcohol's threshold drops with age. The body's water-to-fat ratio shifts as people age, concentrating alcohol in a smaller volume of body water. A drink that barely registers at 50 can produce noticeable impairment at 75, and that impairment stacks on top of every sedating prescription already circulating.
- Grief and isolation reshape the equation. Retirement strips away daily structure. A spouse's death removes the person most likely to notice behavioural changes. Chronic pain grinds on. Some older adults layer alcohol or over-the-counter sleep aids onto existing prescriptions to cope, crossing into polydrug territory without recognizing the shift.
What helps? Annual medication reviews with a pharmacist trained to flag dangerous overlaps. Full disclosure of every substance being taken – prescriptions, over-the-counter pills, supplements, and alcohol. And the willingness to deprescribe. Sometimes, the most protective move a treatment team can make is reducing the pill count rather than adding to it.
How Can You Recognize the Signs of Polysubstance Abuse?
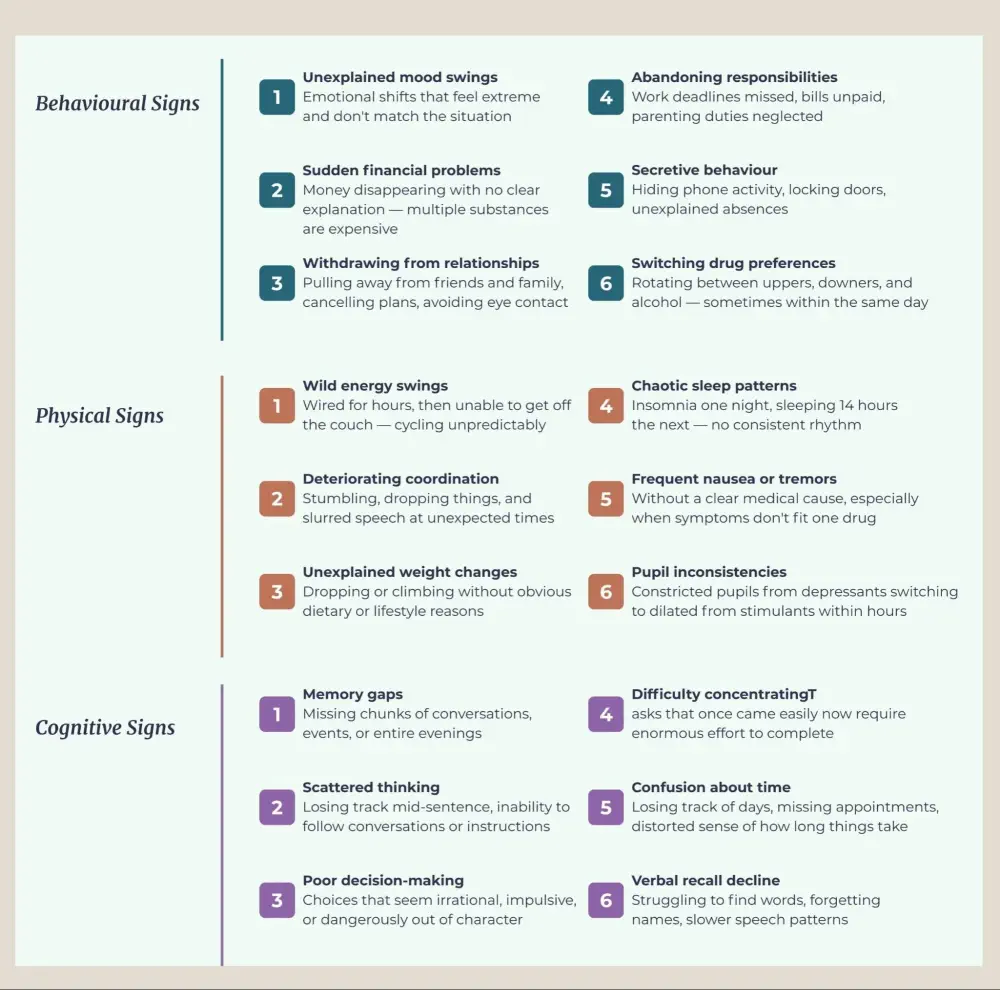
Behaviour unravels first. Unexplained mood swings, sudden financial problems, withdrawing from friends and family, abandoning responsibilities – these patterns emerge before most physical symptoms become visible.
Physically, the signs tend to fluctuate in ways that don't match a single substance. Energy levels swing wildly, wired for hours, then unable to get off the couch. Coordination deteriorates. Weight drops or climbs without an obvious reason. Sleep patterns become chaotic.
The cognitive toll shows up as memory gaps, scattered thinking, and poor decision-making that worsens over time. The key indicator that separates poly-substance use from single-drug misuse: reactions appear inconsistent or disproportionate to what any one substance would produce.
What Does Treatment for Polysubstance Use Disorder Look Like?
Treating polysubstance use disorder means addressing each substance dependency and the motivations that drove the pattern in the first place. Detoxing from one drug but leaving the others untouched makes recovery incomplete and relapse almost guaranteed.
Medically supervised detox comes first. Withdrawal from multiple substances produces overlapping symptoms, some dangerous on their own, potentially life-threatening in combination. Medical teams manage these safely, monitoring heart rate, blood pressure, and breathing around the clock.
Dual diagnosis care tackles co-occurring mental health conditions that tend to fuel polysubstance patterns. Individual and group therapy sessions help unpack why substances got combined and build coping skills that don't involve reaching for another drug.
At the Canadian Centre for Addictions, our programs address every layer of polysubstance dependence – medical detox, one-on-one counselling, and long-term aftercare planning designed to prevent relapse across all substances involved. If you or someone you care about is struggling with polysubstance abuse, call us at 1-855-499-9446.
FAQ
Can mixing prescription drugs count as polysubstance abuse?
Yes. Combining prescribed medications with alcohol, over-the-counter drugs, or recreational substances qualifies as polydrug abuse, even when each medication was legitimately prescribed. Two valid prescriptions that were never meant to overlap can still produce dangerous interactions.
What is the most dangerous drug combination?
Opioids mixed with benzodiazepines or alcohol rank among the deadliest pairings. Naloxone only reverses the opioid component; if benzodiazepines or alcohol are also suppressing breathing, it may not be enough.
How quickly can polysubstance use disorder take hold?
Dependence on multiple substances can form within weeks to months, depending on the drugs involved, dosage, and frequency. Tolerance to one substance often accelerates the slide – once one drug stops working, adding another feels like a logical fix.
Is polysubstance use disorder treatable?
It is. Professional treatment combining medical detox, therapy, and structured aftercare gives people the strongest chance at lasting recovery. Multiple dependencies layered on top of each other make professional support especially valuable.
Does using multiple substances make withdrawal more dangerous?
It can. Withdrawing from several substances at once produces overlapping symptoms, some of which carry serious medical risks on their own. Alcohol and benzodiazepine withdrawal can trigger seizures, and adding opioid withdrawal on top creates a situation that requires round-the-clock monitoring to manage safely.
How can I tell if a loved one is using more than one substance?
Watch for reactions that don't match a single drug. Energy levels that swing wildly, mood shifts that seem disproportionate, or physical symptoms that change unpredictably from day to day can all signal polydrug abuse. Unexplained financial strain and withdrawal from relationships often show up before the physical signs become obvious.
Article sources
- Konefal, S., et al. (2022). "Polysubstance use poisoning deaths in Canada: an analysis of trends from 2014 to 2017 using mortality data." BMC Public Health. Available at: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-022-12678-z
- Canadian Centre on Substance Use and Addiction (2022). "Polysubstance Use and Poisoning Deaths in Canada." CCSA Report at a Glance. Available at: https://www.ccsa.ca/sites/default/files/2022-06/CCSA-Polysubstance-Use-Poisoning-Deaths-Canada-Report-at-a-Glance-2022-en.pdf
- Zuckermann, A.M.E., et al. (2019). "Trends of poly-substance use among Canadian youth." Addictive Behaviors Reports. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6525276/
- Health Canada (2024). "Canadian Student Tobacco, Alcohol and Drugs Survey (CSADS) 2023-24: Key Findings." Government of Canada. Available at: https://www.canada.ca/en/health-canada/services/canadian-student-tobacco-alcohol-drugs-survey/2023-2024-key-findings.html
- Chopra, R., et al. (2025). "Polysubstance use and mental health among young adults." Canadian Journal of Public Health. Available at: https://link.springer.com/article/10.17269/s41997-025-01035-3
- Campeau Calfat, A., et al. (2024). "Association between number of medications and indicators of potentially inappropriate polypharmacy: a population-based cohort of older adults in Quebec, Canada." Journal of Health Services Research & Policy. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11683794/
- Health Canada (2024). "Canadian Postsecondary Education Alcohol and Drug Use Survey (CPADS)." Government of Canada. Available at: https://health-infobase.canada.ca/substance-use/reports/cpads/



