

We offer medical detox and multiple addiction treatment options in our
luxury treatment centres in Port Hope, Cobourg, and Ottawa.
A Guide to Men’s Mental Health

Three out of four Canadians who die by suicide each year are men, yet 67% of Canadian men have never sought professional mental health support. That gap between need and help-seeking sits at the heart of this guide. Men's mental health in Canada looks unlike what most clinical questionnaires were built to detect. The men struggling hardest are usually the ones least willing to say so out loud. This piece is for anyone trying to recognize the signs in himself, or in someone he loves, and to know what to do next.
You'll Learn:
- Which subgroups of Canadian men carry the heaviest burden
- The behavioural cluster clinicians call Male Depressive Syndrome
- Why were standard depression screening tools calibrated against female samples
- How to tell a midlife crisis in men apart from clinical depression
- What does dual diagnosis treatment involve day to day, and what insurance covers in Ontario
How Bad Is the Mental Health Crisis Among Canadian Men?
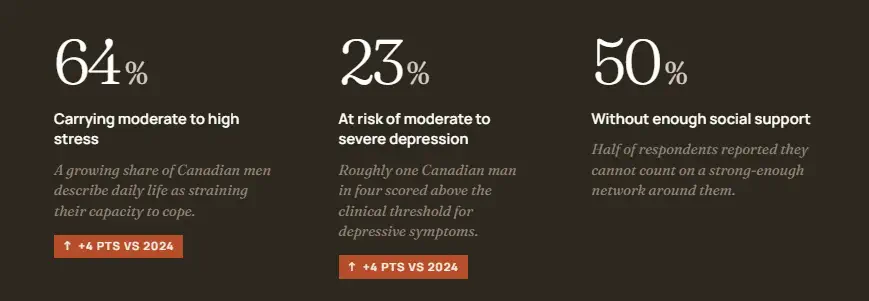
Bad enough that the Canadian Men's Health Foundation's April 2025 survey of 2,000 men recorded a year-over-year worsening across every metric tracked. Stress at moderate-to-high levels reached 64% of men, up four points from 2024. The risk of moderate-to-severe depression hit 23%, also up four percent. Half of the respondents lacked sufficient social support.
Three subgroups carry the heaviest stress load: men living alone reported social isolation at 73%, men aged 19 to 29 at 67%, and racialized men at 59%. Suicide risk follows a separate curve. The Mental Health Commission of Canada identifies First Nations, Inuit and Métis men, military personnel and veterans, and men in occupations with high job stress and access to lethal means as the highest-risk groups. The demographics don't overlap neatly — the most stressed subgroups aren't always the ones at highest suicide risk — but both sets of numbers feed the same crisis.
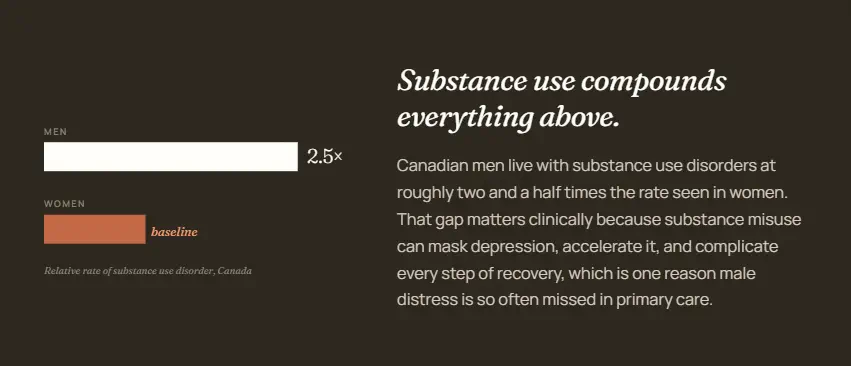
Substance use sits inside the same patterns. Canadian men show roughly 2.5 times the rate of substance use disorders that women do, which makes the clinical signs of distress harder to read.
What Are the Real Signs of Mental Illness in Men?
The behavioural cluster clinicians watch for is called Male Depressive Syndrome, and it sits over the classic depressive core like a layer of camouflage. Each piece looks like a personality trait or bad habit on its own. Together, the signs of mental illness in men form a recognizable pattern.
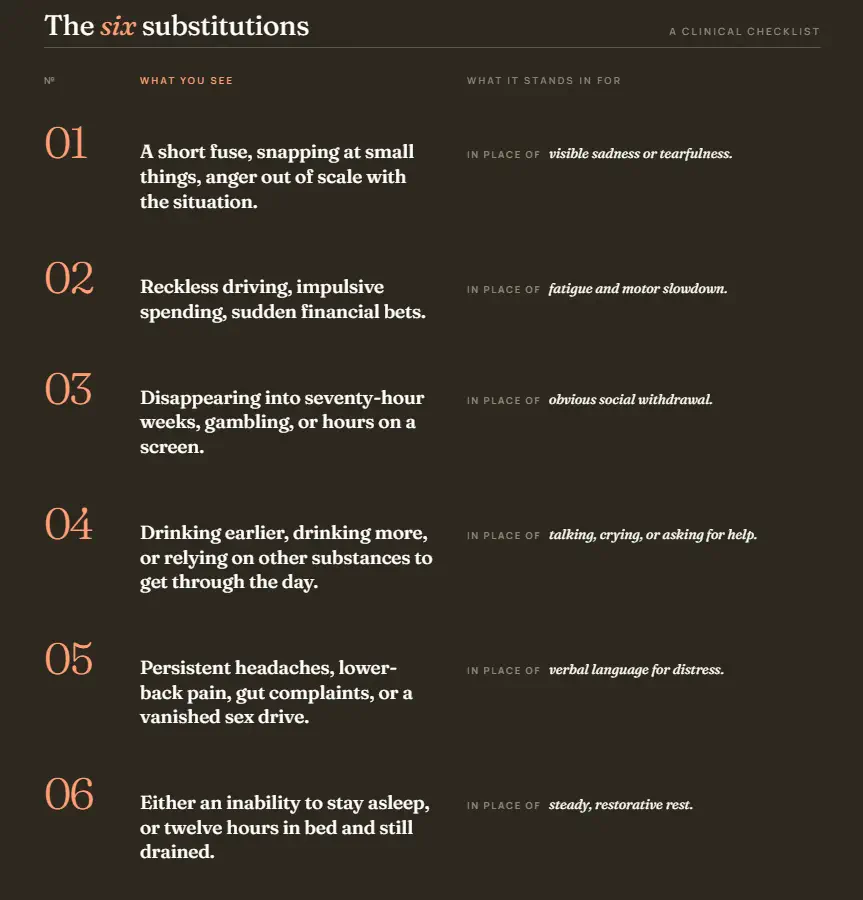
The cluster has six parts:
- Irritability and disproportionate anger replace visible sadness.
- Risk-taking behaviour, including reckless driving and impulsive financial moves, replaces fatigue.
- Escapist overwork, gambling, or compulsive screen use replaces the social withdrawal seen in classic depression.
- Substance misuse, especially alcohol, fills the role that crying or talking might play in another person.
- Headaches, back pain, and loss of libido stand in for emotional language.
- Sleep disturbance shows up as either insomnia or sleeping twelve hours and still feeling depleted.
Duration is what moves the cluster from worrying to clinically meaningful. Guidance suggests that any of these patterns persisting beyond two weeks, or several appearing together, warrants medical attention. Family members usually spot the change before the affected man does, which is why partners, siblings, and close friends are the ones who initiate the first appointment.

What Causes Men's Depression to Look So Different?
Three forces converge to make men's depression present differently.
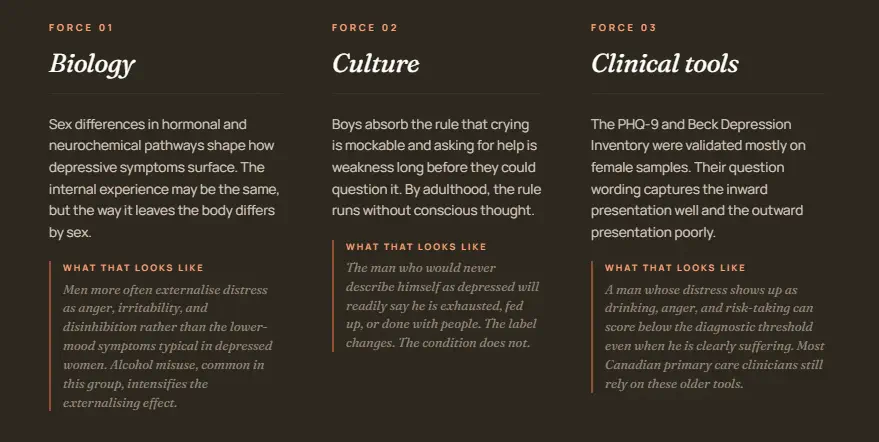
The first is biological. Sex differences in hormonal and neurochemical pathways shape how depressive symptoms surface, with men more likely to externalise distress as anger, irritability, or disinhibition over the lower-mood symptoms typical of depression in women. Alcohol misuse, more common in depressed men than depressed women, amplifies these externalising patterns.
The second force is cultural. Boys learn early that crying invites mockery and that asking for help reads as weakness. Those rules become reflexes by adulthood. The man who would never describe himself as depressed will readily say he is exhausted, fed up, or done with people.
The third force is the diagnostic instruments themselves. Validation studies of the Patient Health Questionnaire-9 and the Beck Depression Inventory drew most of their early data from female samples. Gender-sensitive scales designed in the past two decades, including the Gotland Male Depression Scale and the Male Depression Risk Scale, identify additional cases that the older instruments miss in male populations. In a Canadian validation study, the Male Depression Risk Scale flagged 84.6% of recent suicide-attempt cases among men, compared with 53.9% caught by the standard PHQ-9 cutoff. Most Canadian primary care clinicians still rely on the older tools.
The combined result is documented. Suicide attempt rates between men and women are similar in clinical populations, but Canadian men die by suicide at far higher rates because warning signs are not recognized . Alcohol's role here is mechanistic, not incidental, which is why the drinking and mood connection deserves its own attention.
Is a Midlife Crisis in Men Real or Just a Cliché?
The cliché of the red sports car is mostly Hollywood, but a midlife crisis in men as a clinical phenomenon has real grounding in research. Dartmouth economist David Blanchflower's analysis of 132 countries shows a measurable U-shaped curve in well-being, with the lowest point landing around age 47 in wealthy countries before satisfaction climbs again. Roughly 10 to 20% of men experience this dip as something genuinely disruptive to work, marriage, and identity.
The clinically useful question is how to separate a midlife crisis in men from depression that happens to arrive in midlife. Three markers do most of the work.
| Marker | Midlife Crisis | Depression in Midlife |
| Mood baseline | Restless, hungry for change, sometimes elated | Flat or low across most days |
| Sleep | Disrupted around big decisions, returns when settled | Persistently broken regardless of circumstance |
| Energy | Surges into new pursuits, gym, hobbies, affairs | Depleted even for activities once enjoyed |
A midlife crisis ends when life rearranges around the new direction, usually within two to three years. Depression does not respond to a new car, a new partner, or a geographic move. Andropause, the gradual decline in testosterone from the late thirties onward, complicates this differential by adding fatigue, concentration problems, and lowered libido that overlap with both. The danger window is when a man is making irreversible decisions during the worst of an undiagnosed mood condition. When someone in his forties or fifties suddenly starts drinking heavily, having affairs, or making impulsive financial moves, the question is rarely about the surface behaviour. It is about what the behaviour is trying to solve.

How Do Addiction and Men's Mental Health Feed Each Other?
Research from The Centre for Addiction and Mental Health (CAMH) shows that people with a mental illness are roughly twice as likely to have a substance use disorder compared with the general population. The way substance use shapes psychiatric symptoms varies by drug class, because the wrong substance choice for an underlying condition makes both worse.
Alcohol worsens depression even as it temporarily numbs it.
- Cocaine and methamphetamine deplete dopamine reserves, leaving anxiety and paranoia that can outlast use by weeks.
- Cannabis can blunt anxiety in the short term but is linked to elevated psychosis risk in vulnerable users and worsens depression with prolonged use.
- Opioids flatten emotional range, which is part of why grief, trauma, and untreated men's depression so frequently pull men toward them.
Sequential treatment, where addiction is addressed first and the mental health condition only after sobriety, has weaker outcomes than integrated care for most dual-diagnosis patients.
A man who detoxes from alcohol but leaves his depression untreated relapses because the original pain returns intact. A man on antidepressants who keeps drinking heavily blunts the medication's effect and complicates dose calibration. The dual diagnosis model addresses both conditions in the same room, in the same week, by clinicians who share notes.
What Does the Treatment Look Like for Men in Canada?
Real treatment starts with an assessment that takes the masculine presentation seriously and not as a character flaw to be managed. At the Canadian Centre for Addictions, our admissions team in Toronto inquires how a man is sleeping, what he is drinking, and where his anger is showing up before substance history comes up at all. This establishes honesty and trust about the signs of mental illness in men that more conventional intake conversations miss.
Our residential programs at Hillcrest Mansion in Port Hope and Woodlawn Inn in Cobourg run from 30 to 90 days, with medically monitored detox supervised by three physicians and 24/7 nursing. Daily life includes individual psychotherapy with registered psychotherapists, group work on the reasons men avoid asking for help, and physical recovery time on the lakeside trails. The shoulder-to-shoulder model that the Mental Health Commission of Canada recommends for men, where talking happens during walking, cooking, or working with hands, is built into how the days flow.
For men whose addiction sits on top of an undiagnosed depression or anxiety disorder, our integrated mental health and addiction program handles both conditions at once, under one team.
If something here describes you or a man you love, the first call is the hardest one. Reach us anytime at 1-855-499-9446. You will speak with a human who has heard a version of your story before.
FAQ
How quickly can someone start residential treatment after the first call?
Admission timing depends on bed availability, insurance verification, and medical clearance, but private centres can usually have you start treatment much faster than publicly funded options, where waitlists stretch into months. Our admissions team gives a specific timeline during the first call.
Can a family member arrange treatment without the patient agreeing first?
Admission to residential treatment in Canada requires patient consent in nearly all cases. What family members can do is engage in intervention counselling, which the Canadian Centre for Addictions offers, to help structure a conversation that the patient is more likely to accept.
What happens if symptoms come back after treatment ends?
Lifetime aftercare is included with our residential programs at no extra cost, so a graduate can return to group work, individual sessions, or crisis support indefinitely. Relapse is treated as a clinical event and a signal to intensify support, not a moral failure.
Does taking medication for depression interfere with addiction recovery?
Antidepressants are routinely prescribed during addiction treatment when clinically indicated and do not, in current practice, conflict with recovery. Evidence shows that untreated mood disorders drive a substantial share of relapses.
Will my employer find out if I take medical leave for residential treatment?
Treatment at a private residential centre is covered by physician-patient confidentiality, and short-term disability claims are handled by insurance providers without diagnosis or location being disclosed to the employer. The medical note your physician provides does not name your condition or the treating facility.
Article sources
- Mental Health Commission of Canada. "Men's Mental Health and Suicide in Canada." Mental Health Commission of Canada. https://mentalhealthcommission.ca/resource/mens-mental-health-and-suicide-in-canada-key-takeaways/
- Canadian Men's Health Foundation. "2025 National Men's Health Survey." Canadian Men's Health Foundation. https://menshealthfoundation.ca/press/2025-study-stress-depression-canadian-men/
- Centre for Addiction and Mental Health. "Mental Illness and Addiction Facts and Statistics." CAMH. https://www.camh.ca/en/driving-change/the-crisis-is-real/mental-health-statistics
- Frontiers in Psychiatry. "Gender-Specific Differences in Depressive Behavior." National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8417531/
- Blanchflower, David. "Is Happiness U-shaped Everywhere." National Bureau of Economic Research. https://www.nber.org/papers/w26641
- Rice, Simon. "Validity of the Male Depression Risk Scale in a Representative Canadian Sample." Journal of Mental Health, PubMed. https://pubmed.ncbi.nlm.nih.gov/29271280/




