

We offer medical detox and multiple addiction treatment options in our
luxury treatment centres in Port Hope, Cobourg, and Ottawa.
Why Is Heroin So Addictive

Heroin is one of the most physically dependent substances a person can use. Dependence can take hold within weeks, and the effects of heroin on the brain make stopping without medical support extremely difficult.
Across Canada, thousands of people living with opioid substance use disorder began not with heroin but with prescription painkillers, making the path into dependence less visible until it is already entrenched.
Key Takeaways:
- Why heroin has no legitimate medical use anywhere in the world – and how a major pharmaceutical company spent decades convincing doctors otherwise
- What heroin does to mu-opioid receptors with repeated use – and why that neurological change is what makes stopping feel physically impossible, not a lack of willpower
- Which four risk categories predict who becomes dependent, including one that has nothing to do with the drug itself and everything to do with what came before it
- The three types of signs families miss most — and why each one tends to be mistaken for a completely different problem until several appear at once
- What happens to overdose risk after even two weeks of abstinence – and why this makes specific windows in untreated addiction more dangerous than active daily use
What Is Heroin?
Heroin is an illegal opioid synthesised from morphine, a naturally occurring substance extracted from the seedpod of the opium poppy plant. It is not a medication. It has no approved medical use in Canada and is classified as a Schedule I controlled substance under the Controlled Drugs and Substances Act (the most restrictive category, reserved for substances with high addiction potential and no accepted therapeutic application). The same or equivalent legal status applies in the vast majority of countries worldwide.

This matters because an outdated and inaccurate narrative still circulates: that heroin was once a widely used pharmaceutical and retains some legitimate medical relevance. It doesn't. The drug was briefly marketed in the late 19th century under the trade name "Heroin" by Bayer, who believed it to be a safer alternative to morphine. That belief collapsed within years as its dependence potential became undeniable, and heroin was progressively banned across most of the world throughout the early 20th century.
What Does It Look Like and How Is It Used?
Heroin appears in several forms depending on how it has been processed. Pure heroin is a white powder. Street heroin ranges from brown to off-white, cut with various adulterants. Black tar heroin, common in parts of North America, is dark, sticky, and considerably cruder in composition.
People use heroin by injection, smoking, or snorting. Injection delivers the drug to the brain fastest, which is precisely why it carries the highest addiction risk. All routes produce the same core effects of heroin, but the speed of onset amplifies the neurological reinforcement that drives compulsive use.
The Fentanyl Contamination
Any discussion of heroin in Canada today cannot ignore what has happened to the illicit opioid supply. The street heroin available across most of Canada is frequently contaminated with, or has been entirely replaced by, illicitly manufactured fentanyl and its analogues. Fentanyl is 50 to 100 times more potent than morphine by weight. A dose indistinguishable from heroin to the naked eye can be lethal. This means that every use of street heroin now carries an overdose risk that extends far beyond anything associated with the drug historically.
How Does Heroin Affect the Body?
The speed at which heroin acts on the brain sets it apart from most other opioids and explains why physical dependence can take hold after only a handful of uses. Once heroin enters the bloodstream, it crosses the blood-brain barrier within seconds and is rapidly converted back into morphine. That morphine binds to mu-opioid receptor proteins concentrated in areas of the brain governing pain, reward, and breathing.
Under normal conditions, these receptors respond to the body's own endorphins. Heroin overwhelms that system entirely. Dopamine floods the reward circuits at a volume the brain has never produced on its own. The result is an intense rush of euphoria lasting only minutes, followed by several hours of sedation, slowed breathing, and a feeling of heavy warmth spreading through the body, as users describe.
Short-Term Effects of Heroin
The immediate effects of heroin are not limited to pleasure.
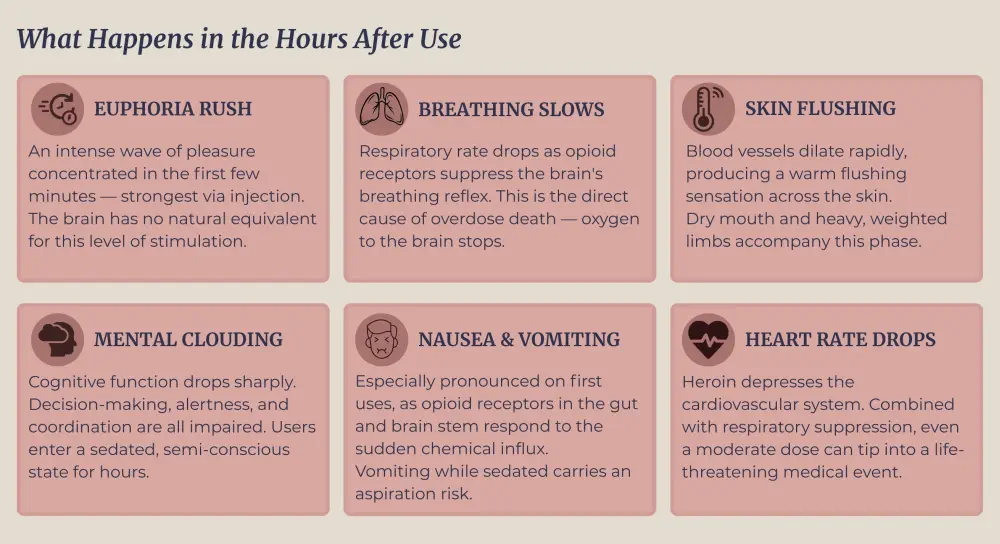
Breathing suppression is the direct cause of heroin overdose death. When the respiratory rate drops too far, the brain is starved of oxygen. Naloxone (sold in Canada as Narcan) can reverse this by displacing heroin from opioid receptors, but it must be administered quickly.
What Repeated Use Does to the Brain
This is where opioid addiction takes root. Each time heroin floods the mu-opioid receptors, the brain responds by reducing its own receptor sensitivity (a protective adjustment that requires progressively larger doses to produce the same effect). This is tolerance, and it develops fast with heroin.
Simultaneously, the brain's natural endorphin production drops. Without the drug, the user no longer feels baseline pleasure, calm, or pain relief. Everyday activities lose their reward value. This neurochemical deficit is one reason withdrawal feels so psychologically brutal. The brain is genuinely depleted, not simply craving a high. The models of addiction that researchers use to explain dependence all converge on this point: repeated opioid exposure rewires the brain's reward circuitry in ways that outlast the drug itself.
Long-Term Neurological and Physical Consequences
Sustained heroin use causes changes that go beyond receptor sensitivity. Neuroimaging research has documented deterioration of white matter in the brains of long-term users, the tissue responsible for decision-making, behavioural regulation, and stress response. These changes do not fully reverse when someone stops using, particularly after years of heavy use.
Physically, the body accumulates damage on multiple fronts:
- Cardiovascular: Injection use scars and collapses veins. Bacteria introduced through shared needles can infect the heart valves, causing endocarditis – a life-threatening condition requiring hospitalisation and, in severe cases, surgery.
- Respiratory: Chronic depression of the respiratory system increases susceptibility to pneumonia and tuberculosis.
- Hormonal: Long-term opioid use suppresses sex hormone production in both men and women, causing reduced libido, menstrual disruption, and infertility.
- Immune: Needle sharing transmits HIV and hepatitis C. Canada's Public Health Agency estimates that injection drug use accounts for approximately 16% of new HIV infections annually.
The body's condition at the point of treatment entry matters. People seeking heroin treatment after years of use carry a heavier burden of co-occurring health problems, and those problems need to be addressed alongside the addiction itself.
What Causes Heroin Addiction?
Not everyone who uses heroin once becomes addicted. That observation is a medical reality with direct clinical implications: certain people carry a substantially higher risk before they ever encounter the drug. Identifying those vulnerabilities is what allows treatment to be personalised rather than generic.
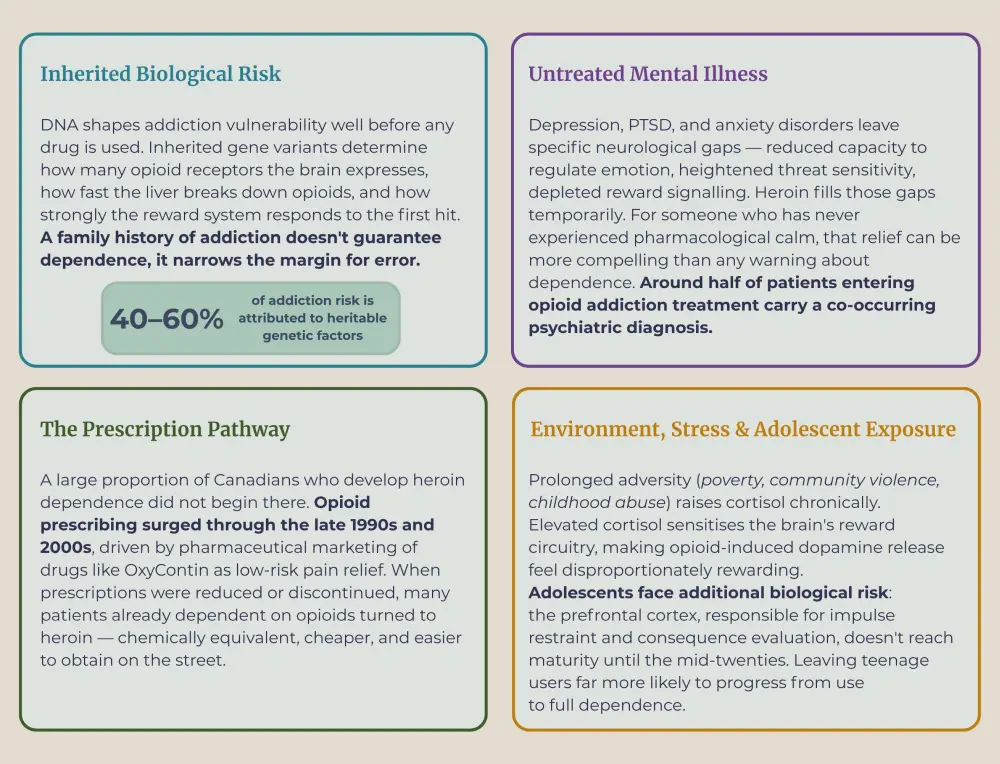
Genetics and Family History
Genetic factors account for roughly 40 to 60 percent of opioid addiction risk. Inherited gene variants determine how densely opioid receptors are expressed in the brain, how quickly the liver metabolises opioids, and how strongly the reward system responds to the effects of heroin on first exposure.
A family history of addiction doesn't guarantee dependence; it narrows the margin for error.
Mental Health and Self-Medication
Depression, PTSD, and anxiety disorders each independently raise the likelihood of heroin use. Heroin suppresses the same neurological distress signals that go unmanaged in undertreated mental illness. For someone without access to effective psychiatric care, that relief can be more compelling than any awareness of dependence risk.
Multiple published studies on narcotic addiction treatment populations found that roughly 50 percent of patients met criteria for at least one co-occurring psychiatric diagnosis at intake. Leaving that diagnosis untreated is one of the strongest predictors of relapse.
The Prescription Opioid Pipeline
Canada's opioid crisis began in doctors' offices, not on the street. Aggressive pharmaceutical marketing throughout the late 1990s and 2000s drove a sharp rise in opioid prescribing. When prescriptions were tightened, patients already dependent on opioids turned to heroin — cheaper, accessible, and neurochemically identical.
According to the Canadian Institute for Health Information, opioid-related harms have reached every province and territory. Many Canadians who currently seek heroin addiction treatment did not begin their opioid dependence with heroin at all.
Environmental and Social Exposure
Early exposure to drug use in the home, among peers, or in high-stress communities substantially raises risk. Adolescents are especially vulnerable — the prefrontal cortex, which governs impulse control and consequence assessment, does not fully mature until the mid-twenties, making teenage use far more likely to progress to dependence.
Chronic stress compounds this. Sustained high cortisol levels sensitise the brain's reward circuitry, amplifying the dopamine response to opioids. Prolonged adversity (childhood abuse, housing insecurity, community violence) creates genuine neurological conditions that heroin temporarily resolves.
What Are the Signs of Heroin Addiction?
The earliest heroin use indicators are easy to dismiss. Fatigue, mood changes, financial problems – each one explainable on its own. The pattern only becomes undeniable once several of these signals appear together, by which point dependence is already entrenched. Recognising what to look for, and when, closes that gap.
Physical Signs of Heroin Addiction
The body produces visible evidence of opioid dependence before most people acknowledge it.
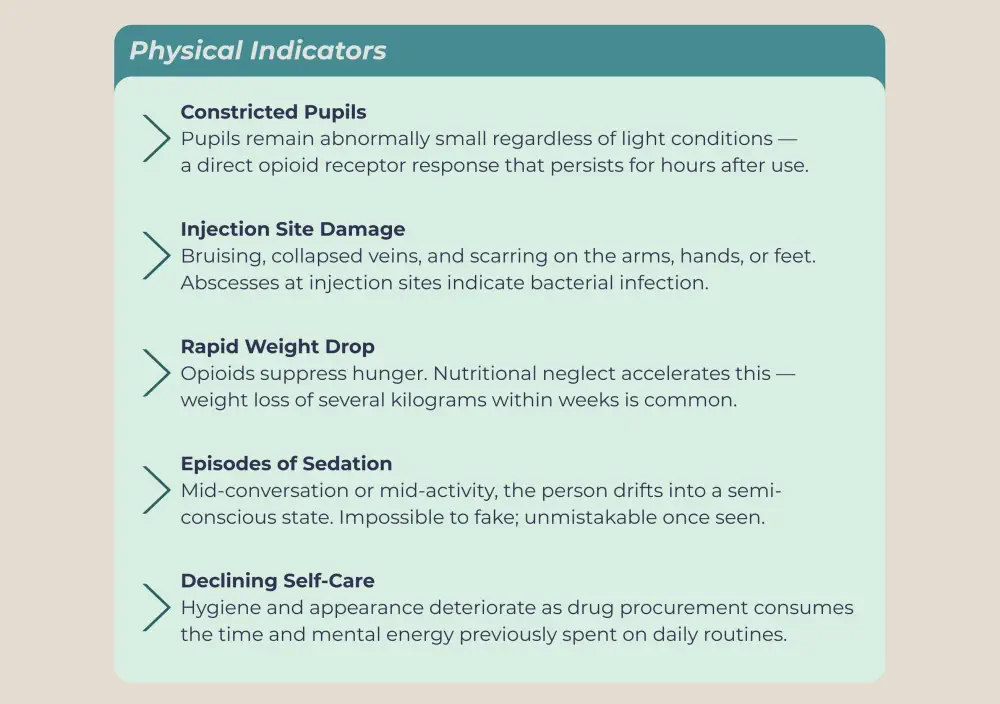
Some of these appear within weeks of regular use. The physical deterioration, like weight loss, skin damage, and visible vein scarring, accumulates over months.
Behavioural Signs
Behaviour shifts before physical deterioration becomes obvious.
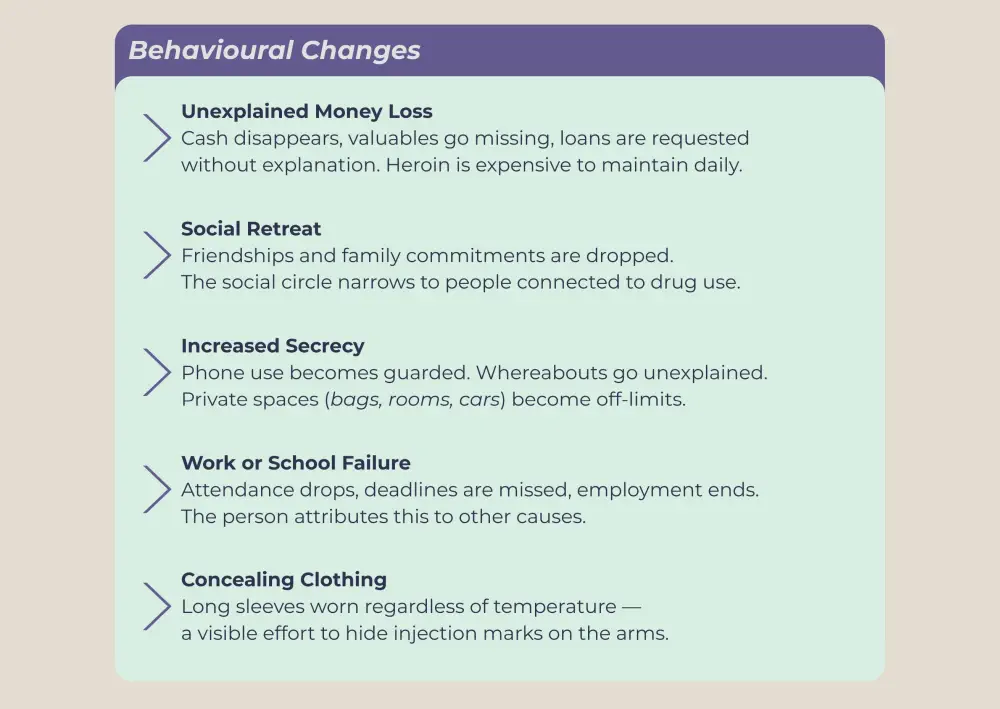
Families frequently attribute these changes to depression, relationship breakdown, or financial stress. That misreading delays intervention by months or years, and the addiction deepens in that gap.
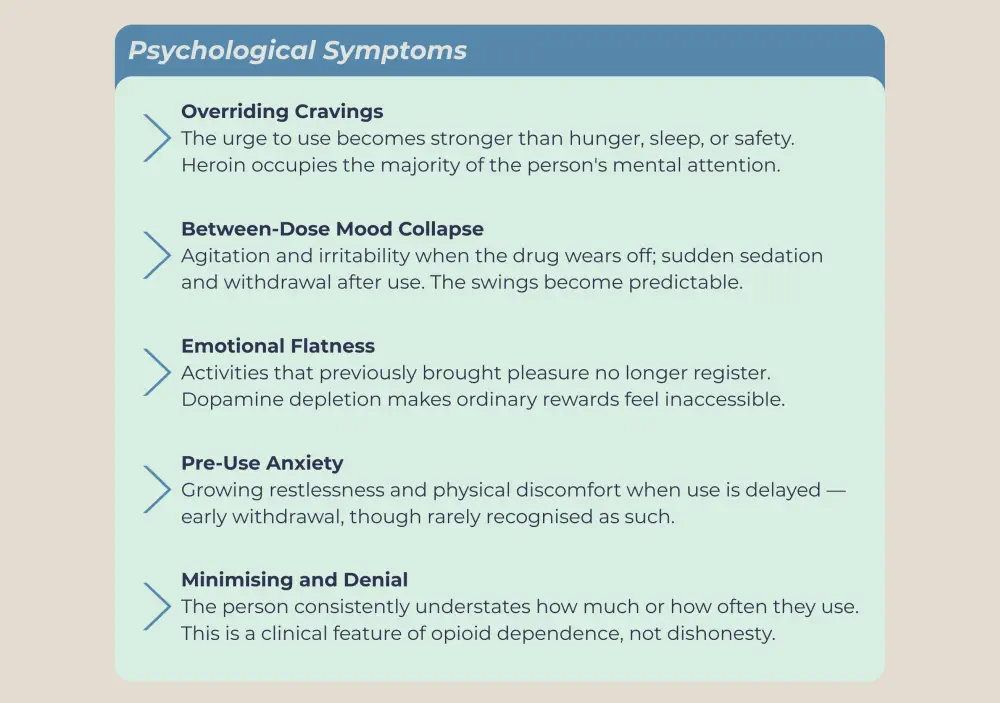
Psychological Heroin Addiction Symptoms
Less visible but equally telling.
Where Clinical Diagnosis Begins
The DSM-5 defines opioid use disorder, the diagnostic term for opioid addiction, as two or more of eleven specific criteria occurring within twelve months. These include using larger amounts than intended, failed attempts to reduce use, continued use despite harm to health or relationships, and withdrawal on cessation.
Two to three criteria indicate a mild disorder. Six or more points indicate severe addiction requiring immediate professional intervention. The threshold matters because it determines the level of treatment for heroin use disorder required, whether detoxing under medical supervision is enough, or if you need to go to a residential treatment center.
One point bears stating directly: a person does not need to reach a crisis before the diagnostic threshold is crossed. Someone using heroin daily for three months, missing work, and concealing use from family has already met the criteria. Early-stage heroin dependency signs carry the same clinical weight as late-stage ones, and respond better to treatment at that point.
What Does Heroin Treatment Look Like?
Heroin treatment is not a single event. It is a sequence of medical and therapeutic interventions, each targeting a different layer of dependence – the physical, the neurochemical, and the psychological. No single component works in isolation. The evidence consistently shows that outcomes are substantially better when all three are addressed simultaneously and in a structured setting.
Medical Detox: The First 7–10 Days
Withdrawal peaks within 48 to 72 hours and runs its course over seven to ten days. Medically supervised detox keeps the person safe through that window, using medications to manage muscle pain, nausea, insomnia, and cardiovascular instability. It clears the physical dependence. The neurochemical and psychological work begins after.
Opioid Agonist Therapy
Opioid agonist therapy is the most evidence-supported pharmacological intervention for opioid drug addiction. Two medications anchor this category:
Methadone is a long-acting opioid agonist taken orally once daily. It binds to the same mu-opioid receptors as heroin, preventing withdrawal and eliminating cravings without producing a euphoric high at therapeutic doses. Decades of outcome data show that methadone maintenance reduces illicit opioid use, lowers overdose mortality, and improves retention in treatment.
Buprenorphine/naloxone (Suboxone) is a partial agonist. It activates opioid receptors at a ceiling level, meaning higher doses do not produce proportionally greater effects. This ceiling limits overdose risk. The naloxone component deters injection misuse by triggering withdrawal if the medication is injected; it must be taken sublingually as prescribed to function correctly.
Both medications are approved for use in Canada and can be prescribed by certified physicians in office-based settings. Both are designed to stabilise the person neurochemically so that therapeutic work becomes possible.
Behavioural Therapy
Cognitive behavioural therapy identifies the triggers and behavioural sequences that precede use and replaces automatic responses with deliberate alternatives. Individual counselling addresses trauma and co-occurring mental illness. Group therapy provides contact with people at different stages of recovery, reducing isolation and demonstrating that sustained abstinence is achievable.

Inpatient vs. Outpatient Care
Outpatient programs suit people with mild to moderate dependence and a stable home environment. Residential care is warranted when dependence is severe, when the home contains active triggers, or when prior outpatient attempts have not been successful.
At the Canadian Centre for Addictions, residential programs run from 30 to 90 days across our facilities in Port Hope and Cobourg, with three physicians on staff and lifetime aftercare following discharge.
If you are ready to take the first step, contact us at 1-855-499-9446.
The Longer Heroin Abuse Goes Unaddressed, The Narrower the Window Gets
Heroin addiction is not a character failure that resolves with sufficient willpower, and it is not a death sentence that resolves only in one direction. It is a medical condition with a documented biology, a predictable progression, and treatments that work, but those treatments work best when they reach a person before the overdose risk escalates, before relationships collapse beyond repair, and before years of neurological adaptation make recovery harder to sustain.
The evidence consistently shows that early intervention produces better outcomes than late intervention across every measure: retention in treatment, long-term abstinence, health recovery, and social reintegration. The barrier is rarely a lack of available care. It is the gap between recognising that heroin dependency signs are present and accepting that professional heroin treatment is what the situation actually requires.
If someone you know is showing the signals covered in this article, that recognition itself is the point of action, not a reason to wait and see.
FAQ
How quickly can someone become addicted to heroin?
Physical dependence can take hold within two to three weeks of daily use. The speed depends on route of administration, individual genetic factors, and dose. Injection produces dependence faster than snorting or smoking.
What are the most dangerous symptoms of heroin dependence to watch for?
Respiratory depression during use and the tolerance drop after any period of abstinence are the two highest-risk situations. A person who has gone several days without heroin, voluntarily or not, faces a sharply elevated overdose risk if they return to their previous dose.
Is heroin withdrawal life-threatening?
In otherwise healthy adults, opioid withdrawal is rarely fatal on its own. The real danger is the return to use it drives, most people cannot tolerate the seven to ten days of peak symptoms without medical support, and relapsing during withdrawal onto a dose the body no longer tolerates is when overdose deaths occur.
What is the difference between opioid addiction and heroin addiction?
Heroin addiction is a specific form of opioid addiction. Both involve dependence on substances that bind to mu-opioid receptors, and both are treated with the same medications – methadone, buprenorphine, and naltrexone. The distinction matters mainly in the context of how dependence developed, not how it is treated.
How effective is heroin treatment at a residential centre?
Residential heroin recovery programs consistently outperform outpatient-only care for people with severe dependence. At the Canadian Centre for Addictions, our programs carry a 95.6% success rate, supported by three on-staff physicians, program lengths from 30 to 90 days, and lifetime aftercare following discharge.
Article sources
- Sneader W. (1998). "The discovery of heroin." The Lancet, 352(9141), 1697–1699. Available at: https://pubmed.ncbi.nlm.nih.gov/9853457/
- Li W., Chen Z., & Yu J. (2019). "Opioid Addiction, Genetic Susceptibility, and Medical Treatments: A Review." International Journal of Molecular Sciences, 20(17), 4294. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6747085/
- Yuan K., Qin W., Liu J., Guo Q., Dong M., Sun J., Zhang Y., Liu P., Wang W., Wang Y., Li Q., Yang W., von Deneen K. M., Gold M. S., Liu Y., & Tian J. (2013). "Progressive White Matter Microstructure Damage in Male Chronic Heroin Dependent Individuals: A DTI and TBSS Study." PLoS ONE, 8(5), e63212. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC3641135/
- Rogers A. H., Shepherd J. M., Orr M. F., & Farris S. G. (2022). "Prevalence of mental disorders among people with opioid use disorder: A systematic review and meta-analysis." Drug and Alcohol Dependence, 238, 109551. Available at: https://pubmed.ncbi.nlm.nih.gov/35797876/
- Vo H. T., Imani-Hashemi A., & Ait-Daoud Tiouririne N. (2024). "Opioid Use Disorder: Evaluation and Management." StatPearls. Available at: https://www.ncbi.nlm.nih.gov/books/NBK553166/
- Public Health Agency of Canada. (2025). "Opioid- and Stimulant-related Harms in Canada." Special Advisory Committee on the Epidemic of Opioid Overdoses. Available at: https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/
- Public Health Agency of Canada. (2024). "HIV in Canada, Surveillance Report to December 31, 2023." Available at: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/hiv-canada-surveillance-report-december-31-2023.html



